The headlines say it all. These are the results so far of adverse reactions to various medications and vaccines according to the official VAERS reporting, which give low estimates. The truth is worse. This is from Sen John Johnson:
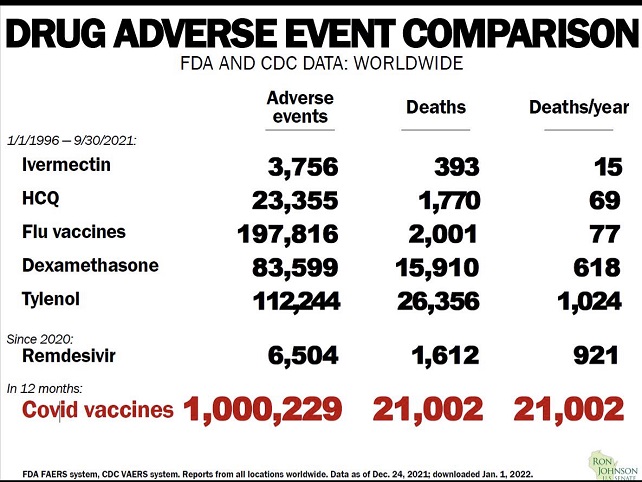
It should be noted that for the first five medications the time frame is nearly 16 years, the result for COVID vaccine is one year.
Of all medications that actually works against COVID with a more than 75% efficiency, Ivermectin has been approved for human use against river blindness and other parasites, such as head lice since late 1980’s. The countries in Africa that routinely use it for parasite control have a COVID case and death rate of less than 1/10th of the countries in Africa that don’t. There are almost no adverse reactions.
HCQ is almost as good COVID fighter as Ivermectin when taken early in conjunction with Zinc. It’s effectiveness is at least 65% and has been used for over 50 years as an anti malaria drug, against lupus and some rheumatoid diseases. It is given to pregnant women and nursing mothers without restrictions.
Flue vaccines have very few adverse effects, but they happen.
Remdisivir was approved very fast, after all, it was expensive and showed early promising results, but it turned out that nearly 30% of the test clientele had used HCQ before entering the protocol. It turned out, that without HCQ it was not so good after all.
Alone in the history of vaccines has COVID vaccines been approved with such a staggering rate of adverse reactions and over 20,000 deaths from the vaccine in a year. Yet it helps people at risk, people over 60, obese, diabetic, anemic, vitamin C and D deficiency, immune compromised, high blood pressure and a variety of diseases, so they were important in the beginning of the disease, and will be for a while until the therapeutics are approved.
In the mean time , children and young adults without additional risk factors are at higher risk of dying if they take the vaccine than if they get COVID, older people should still go the vaccine route. With admittedly limited statistics available I have calculated the crossover point to be 45 years for people without additional risk factors.

First of all, note that the “adverse event” reporting systems make no attempt to establish causality. They track adverse events which occur soon enough after a jab that someone thought it plausible that the two things could be connected. But it is not correct to say there have been “over 1 million adverse reactions to COVID vaccines.” Rather, you should say that there have been over 1 million adverse events which occurred soon after a Covid-19 jab.
That might not sound like a big difference, but it is. To understand why, let’s do some math.
Adverse events happen to people all the time. Only if there were an unexpectedly high number of some type of adverse event occurring soon after vaccination would that be evidence that the vaccine jabs were causing the adverse events. So to make that determination we need to know the expected number of adverse events not caused by the jabs.
The easiest adverse event to find good statistics for is deaths. So let’s work with that.
Each day, when there’s nothing extraordinary going on, like a pandemic, a little more than 0.002% of the world’s population dies. (The USA has an older than average population, so the percentage is a bit higher here; in 2019 it was 0.00238%.)
There’ve been 9.28 billion Covid-19 vaccine jabs given so far, globally. So we should expect that a little more than 0.002% of 9.28 billion people have died within one day of getting a Covid-19 vaccine jab, and a bit more than 7 times 0.002% of 9.28 billion people have died within one week of a Covid vaccine jab, of causes unrelated to the jab.
(Actually, the vaccine jabs have been given preferentially to older people, and disproportionately in countries with older-than-average populations, so the real numbers should be a bit higher than that, but for simplicity I’ll ignore that.)
7 times 0.002% of 9.28 billion = 1.3 million deaths
That’s a lowball estimate of the number of people who can be expected to have died within one week of getting a Covid-19 vaccination jab, of causes completely unrelated to vaccination, even if there were no pandemic going on, and even if the vaccines actually caused no adverse events at all.
So you can see why U.S. VAERS statistics, and similar data from other countries, are not giving evidence that the vaccine events are causing deaths or other adverse events.
My main point referencing VAERS was to compare the relative safety and risk of adverse reactions with Ivermectin and HCQ compared to the vaccines. Ivermectin is taken as a regular prophylactic and therapeutic against parasites by nearly 2 billion people since the late 80’s. It is advised to take a limited dose of Ivermectin upon entry to this country from the Middle East, parts of Africa and Latin and South America, including entry trough the Southern border. HCQ has been taken for over 50 years as a malaria drug and is also used against LUPUS and some forms of rheumatism, totaling billions of doses. Yet I remember Cavuto on Fox saying, after having an M.D. telling how dangerous it is, and I quote “if you take this and have any heart issues YOU WILL DIE! It is my opinion, shared with a large group of concerned doctors that care about people, that if we had approved these drugs as a prophylactic and early (the first 5 days) therapeutic, 80% of the current deaths from COVID would have been avoided. Vaccines are good for people over 45 and with special risk factors, but as far as the Omicron variant vaccinated people have a higher risk of contracting the disease and are also stronger transmitters of it.