Denmark has a very good medical system for all. It is universal and medication needs are met as determined by the medical professionals and government. This is their official message:
And it is about time. The data all over the world is showing that the COVID vaccines do more harm than good for people under 50. In U.K. the February COVID-19 deaths were 90% from vaccinated people, making the vaccinated death rate at least twice as high as from the un-vaccinated, see results here. This was clear a year ago in U.S. as well, see here. Since then it has been clear that only very vulnerable people under the age of 45-60 should be boosted or even vaccinated.
On Saturday, September 10, 2022 top doctors from across India met virtually with doctors from 34 countries to sign a Declaration of International Medical Crisis.
We, the medical doctors and scientists from all over the world, declare that there is an international medical crisis due to the diseases and deaths co-related to the administration of products known as “COVID-19 vaccines”.
We are currently witnessing an excess in mortality in those countries where the majority of the population has received the so called “COVID-19 vaccines”. To date, this excess mortality has neither been sufficiently investigated nor studied by national and international health institutions.
The large number of sudden deaths in previously healthy young people who were inoculated with these “vaccines”, is particularly worrying, as is the high incidence of miscarriages and perinatal deaths which have not been investigated.
A large number of adverse side effects, including hospitalisations, permanent disabilities and deaths related to the so-called “COVID-19 vaccines”, have been reported officially. The registered number has no precedent in world vaccination history.
Examining the reports on CDC’s VAERS, the UK’s Yellow Card System, the Australian Adverse Event Monitoring System, Europe’s EudraVigilance System and the WHO’s VigiAccess Database, to date there have been more than 11 million reports of adverse effects and more than 70,000 deaths co-related to the inoculation of the products known as “covid vaccines”. We know that these numbers just about represent between 1% and 10% of all real events.
Therefore, we consider that we are facing a serious international medical crisis, which must be accepted and treated as critical by all states, health institutions and medical personnel worldwide.
Therefore, the following measures must be undertaken on an urgent basis:
A worldwide ‘stop’ to the national inoculation campaigns with the products known as “COVID-19 vaccines”.
Investigation of all sudden deaths of people who were healthy previous to the inoculation.
Implementation of early detection programmes of cardiovascular events which could lead to sudden deaths with analysis such as D-dimer and Troponin, in all those that were inoculated with the products known as “COVID-19 vaccines”, as well as the early detection of serious tumours.
Implementation of research and treatment programmes for victims of adverse effects after receiving the so called “COVID-19 vaccine”.
Undertaking analyses of the composition of vials of Pfizer, Moderna, Astra Zeneca, Janssen, Sinovac, Sputnik V and any other product known as “COVID-19 vaccines”, by independent research groups with no affiliation to pharmaceutical companies, nor any conflict of interest.
Studies to be conducted on the interactions between the different components of the so called “COVID-19 vaccines” and their molecular, cellular and biological effects.
Implemention of psychological help and compensation programmes for any person that has developed a disease or disability as a consequence of the so called “COVID-19 vaccines”.
Implemention and promotion of psychological help and compensation programmes for the family members of any person who died as a result of having been inoculated with the product known as “Covid-19 vaccines”.
Consequently we declare that we find ourselves in an unprecedented international medical crisis in the history of medicine, due to the large number of diseases and deaths associated with the “vaccines against Covid-19”. Therefore, we demand that the regulatory agencies that oversee drug safety as well as the health institutions in all countries, together with the international institutions such as the WHO, PHO, EMA, FDA, UK-MHRA and NIH respond to this declaration and act in accordance with the eight measures demanded in this manifesto.
This Declaration is a joint initiative of several professionals who have been fighting for this cause. We call on all doctors, scientists and professionals to endorse this statement in order to put pressure on the entities involved and promote a more transparent health policy
This is almost the same result that was available for anyone to see in death rates for people taking ivermectine regularly against river blindness in sub-saharan Africa versus the people living in the rest of Africa:
The explanation given by CDC and others was that these statistics are not done scientifically with double blind control groups and the medical care in these country is inferior and many cases go undiagnosed and so the results are unreliable. However, they too signal a 90+ percent reduction in death rates from COVID. One caveat: Sub-saharan Africa has a much younger population than the rest of the world.
Conclusion: Every day ivermectine treatment is not approved cost lives. 90% of the COVID deaths could be avoided by just approve the drug to treat early COVID, a drug that is already approved for other purposes, and in some case mandated for about 2.4 billion people.
When a critical mass of American people realize what has been done to them, there will need to be a reckoning.
By Debra Heine
March 4, 2022
In recent weeks, there have been several stunning revelations concerning the COVID-19 mRNA vaccines—and they are being all but ignored by a corporate media eager to change the subject.
The FDA on Tuesday released a large tranche of Pfizer clinical trials documents in response to a Freedom of Information (FOIA) request by the Public Health and Medical Professionals for Transparency. The documents show that the company knew people were at risk of experiencing more than 1,000 unique adverse side-effects to the mRNA injections.
Additionally, scientists last week revealed that Pfizer’s COVID-19 vaccine can enter human liver cells and be converted into DNA—something the fact-checkers and the U.S. Centers for Disease Control assured the public could never happen. Scientists also recently discovered that a sequence of genetic material patented by Moderna in 2018 bears a suspicious similarity to the spike protein in Sars-Cov2.
And a new study published on March 2 found that the synthetic mRNA found in the vaccines does not degrade quickly as promised, but continues to produce spike proteins for nearly two weeks.
Amid these new discoveries, the medical establishment won’t stop pushing the genetic vaccines that have failed to stop the coronavirus.
The COVID pandemic now plays second fiddle to the Russia-Ukraine war in the media, but the virus continues to rage through highly vaccinated countries, afflicting the triple-vaxxed most of all.
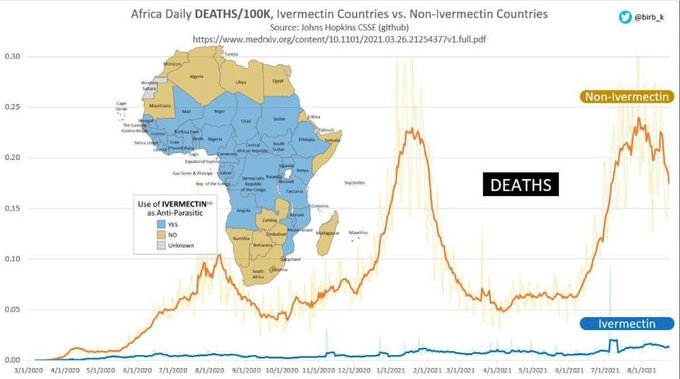
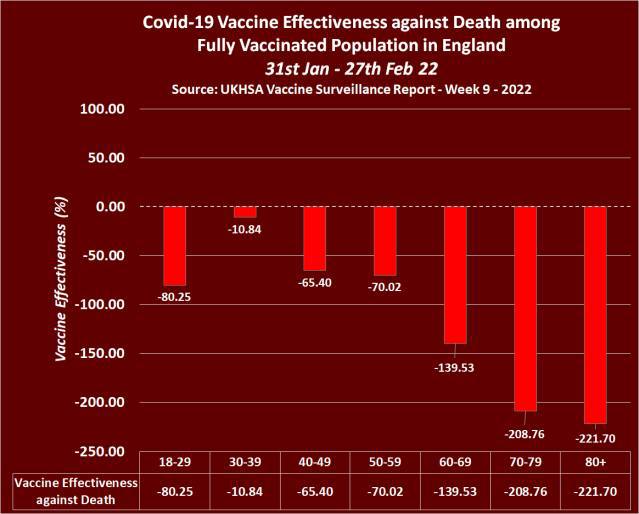
In the United Kingdom, only 394 vaccine-free persons died in weeks 5-8 of 2022, compared to the 3,527 who were vaccinated, according to the UK Health Security Agency. This means unvaccinated Brits only comprised 10 percent of all COVID deaths during those weeks.
The effectiveness of the vaccine is shown in this chart
In other words, if you are over 70 years old your risk of dying from COVID is more than three times as large if you are vaccinated. It’s no wonder Pfizer wanted to hide the data for 75 years.
“This is a bombshell,” said Children’s Health Defense (CHD) president and general counsel Mary Holland. “At least now we know why the FDA and Pfizer wanted to keep this data under wraps for 75 years. These findings should put an immediate end to the Pfizer COVID vaccines. The potential for serious harm is very clear, and those injured by the vaccines are prohibited from suing Pfizer for damages.”
It contains more revealing data about the “safety” of the “vaccine”, well worth a second look. The article also shed some light on the Moderna patent that was issued three years prior to the outbreak of COVID-19. That was the reason a vaccine was ready to be tested one week after getting the warp speed go-ahead to develop a vaccine. The “Warp Speed” component was a promise to buy the vaccine in large quantities, whether it worked or not, thus eliminating the production ramp up. This also eliminated the economical and legal risk for the pharmaceutical companies. By not evaluating and acting on the results from the emergency use of the vaccine the Pharmaceutical companies are responsible for a large number of COVID deaths by vaccine. By reducing the immunity level of the vaccinated there are also an increase in the number of non vaccine related deaths; yet to be published.
A large medical study of seniors, both Viagra users and non users (7.2 million seniors medical records were scanned for six years by the Cleveland Clinic) and they found that Viagra users were 69% less likely to develop Alzheimer disease. This was interesting. Did they find anything else? Less Cancer, less Parkinson’s disease?
Could there be something else that made a difference? Viagra itself was developed to be a blood pressure lowering drug by expanding the blood vessels. During the early trials they found that it had some unexpected side effects. For some, the side effects were desirable, so they repurposed the drug, and Pfizer racked up about 15 Billion dollars in sales until the patent expired in 2020. It is now generic under the name sildenafil. There is only one problem with this. To repurpose a drug, in this case against Alzheimer you have to have a control group that is not aware that they are given a placebo, which is not possible in this case. Plus it is now generic, so there is no interest in doing a double blind study for economic reasons, it no longer fits the medical industry’s business model.
Many years ago I saw a nicely framed plug for flossing in my dentist’s office. It said: People who floss every day live on average seven years longer. This may very well be true, but could it also be because people who floss take care of themselves in many other ways?
A long time ago there was a study that established a strong correlation between circumcision and prostate cancer. People who were not circumcised had a much higher incident of prostate cancer, case closed, get circumcised. There was only one problem with the study: It was taken mostly in Minnesota with a large Scandinavian population. Scandinavians do not get circumcised as a rule, and they are genetically much more prone to get prostate cancer than other people. When the genetic variations are taken out, there is no difference between circumcision, non circumcision and cancer.
Which brings me to COVID-19 and why more pigmented people are more likely to suffer, even die from COVID-19. The first excuse is that they get an inferior health care because we are a deeply racist society. There are a couple of other possibilities. An Indonesian study showed a strong correlation between Vitamin D levels and fatal outcome for older people with COVID-19. If the level was below 27 ng/ml the death rate was over 80%, if the level was over 31 ng/ml the death rate was less than 10%. See: https://lenbilen.com/2020/12/27/vitamin-d-as-covid-19-fighter-a-most-important-virus-fighter/
Another possibility is there are genetic differences between people of dark complexion and pale-skinned people. It is through genetic differences we determine our ancestry, it has become widely popular, so it is not in and of itself racist to look into one’s roots. It turns out that the rate of COVID-19 in equatorial Africa is much lower than in U.S. In Africa there was a debilitating illness called river blindness. The parasite killer Ivermectin, originally developed against parasites in horses and as heart worm killer in dogs proved effective against river blindness, and so it became widely distibuted in Central Africa. The countries that use Ivermectin have around one tenth of the cases than the countries of North and Southern Africa. It seems that Ivermectin had been inadvertently repurposed to fight COVID-19. See: https://lenbilen.com/2020/12/27/vitamin-d-as-covid-19-fighter-a-most-important-virus-fighter/
To test this hypothesis Indonesia, India and Japan did introduced Ivermectin as the primary early prophylactic and therapeutic COVID-19 fighter. The results are startling, Indonesia has seen new cases drop 99.5% and deahs drop 99.4% since the peak before introduction of Ivermectin. The corresponding numbers for India are 98% and 93.3%, but in Uttar Pradesh and Delhi the results are much better. In Japan the cases are down 99.5% and deaths are down 98.4%.
Can the U.S. achieve similar successes by repurpose Ivermectin to fight COVID-19? It is a strong virus killer, and it is more broadband than the mRNA vaccines. The vaccines work too as a Prophylactic Therapeutic for a season, but is what they call leaky insofar that they are more specific and make possible an occasional vaccine resistant mutation to develop, and so a vaccine booster variant has to be developed and distributed, thus satisfying the medical industry’s business model, first do not cure the patient, but maintain stable control and assure the patient of a long life of dependency.
The other buisness model advocared by the medical doctors and nurses is that they really want to cure the patient. Ivermectin will go a long way to achieve that goal. Just think, reducing COVID hospitalizations and deaths by a modest 90% in about seven weeks after Ivermectin is fully approved would change things.
This document provides an integrated analysis of the cumulative post-authorization safety data, including U.S. and foreign post-authorization adverse event reports received through 28 February 2021.
The document reveals that within just 90 days after the EUA release of Pfizer’s mRNA vaccine, the company was already aware of voluntary adverse reaction reports that revealed 1,223 deaths and over 42,000 adverse reports describing a total of 158,893 adverse reactions. The reports originated from numerous countries, including the United States, United Kingdom, Italy, Germany, France, Portugal, Spain and other nations.
Of special interest is what happens to pregnant and breastfeeding mothers
This is alarming, since a gestation period is 9 months, and these are snapshots the first 90 days after introducing the vaccine. The question that many women have, especially health care women that have seen what is going on is: How safe is this vaccine really? Will it cause infertility? Will it drastically increase stillbirth? Will it damage my child in the womb? We now have nearly a year of data, and no one comes out and assures us that none of these things are happening, just an increase in deaths, and a large number of adverse reactions.
The second set of questions are: How much worse is COVID-19 itself compared to the vaccine? Does COVID-19 cause infertility? Is blood clotting worse? It maybe that for children and young adults the vaccine is worse than COVID itself, other data seems to suggest so for people under 45 years of age.
This vaccine should be halted for people under age 45 until answers are given. There seems to be a benefit for older people, a substantially reduced death risk.
BNT162b2 5.3.6 Cumulative Analysis of Post-authorization Adverse Event Reports CONFIDENTIAL Page 1 APPENDIX 1. LIST OF ADVERSE EVENTS OF SPECIAL INTEREST 1p36 deletion syndrome; 2-Hydroxyglutaric aciduria; 5’nucleotidase increased;
Bad news about the dangers that mRNA vaccines may pose to the heart and blood vessels keeps coming.
A new study of 566 patients who received either the Pfizer or Moderna vaccines shows that signs of cardiovascular damage soared following the shots. The risk of heart attacks or other severe coronary problems more than doubled months after the vaccines were administered, based on changes in markers of inflammation and other cell damage.
Patients had a 1 in 4 risk for severe problems after the vaccines, compared to 1 in 9 before.
Dr. Steven Gundry, a Nebraska physician and retired cardiac surgeon, presented the findings at the Scientific Sessions of the American Heart Association’s annual conference in Boston last week. An abstract is available in Circulation, the AHA’s scientific journal.
My conclusion from that statistics is that vaccines are beneficial if you are over the age of 46. Because of the coarseness in the age-related data, only 4 categories, the uncertainity is +- 5 years. This is one more argument that speaks for the conclusion that if you are young, you are better off getting COVID-19 and acquiring natural immunity, rather than take the vaccine and be stuck with booster shots every 6 to 8 months. The vaccine itself is experimental, and we do not yet know the long term effect of it, much less the long term effect of the booster shots.
Vaccinated English adults under 60 are dying at twice the rate of unvaccinated people the same age
And have been for six months. This chart may seem unbelievable or impossible, but it’s correct, based on weekly data from the British government. The brown line represents weekly deaths from all causes of vaccinated people aged 10-59, per 100,000 people. The blue line represents weekly deaths from all causes of unvaccinated people per 100,000 in the same age range. This graph is correct. Vaccinated people under 60 are twice as likely to die as unvaccinated people. And overall deaths in Britain are running well above normal. The basic data is available here, download the Excel file and see table 4:
This new data set indicates a sharp rise in overall mortality from all cases as people get older it was given as 2 categories, unvaccinated and those having received 2 doses of vaccine, broken up in 10-60, 61-70, 71-80, and 80+ years age groups, coarse but usable categorization. This indicates a decrease in deaths of 45% for people 61-70, 46% for the age group 71-80, and 33% for people 80 and over. All these numbers jump widely so the confidence interval is only about 10%. Massaging the data as best I could with this limited set I came up with the age of 46 years as the crossover point, above which vaccines are preferable.
The conclusion is this: People over the age of 46 should be encouraged to get vaccinated, people under the age of 46 should only get vaccinated if they are in the vulnerable category, and only with a physician’s recommendation.
This picture was displayed at a Monday July 6 White House press conference. White House press secretary Kayleigh McEnany told reporters that the American death toll has fallen for weeks and the virus fatality rate is below France, the United Kingdom and Germany.
She said the death toll has significantly dropped from the height of the outbreak when the U.S. logged 2,500 deaths per day to 254 deaths on Saturday July 3, according to the article.
To confirm it the case fatality rate for Germany is as of July 15: 4.54 %
The case rate for the world is 4.24%
The corresponding number for U.S.A.: 3.83%
Is that the lowest percentage in the world?
There are more than ten countries with a lower case fatality rate. At least ten of them have one thing in common. These ten countries prescribe the use of HydroxyChloroQuine to all people that show symptoms of COVID-19, even before a positive test is confirmed.
Turkey: 2.51%
South Korea: 2.14%
Senegal: 1.87%
Morocco: 1.58%
Russia: 1.60%
Malaysia: 1.39%
United Arab Emirates: 0.60%
Costa Rica: 0.44%
Bahrain: 0.34%
Qatar: 0.14%, but since 88% of the population are migrant workers between 20 and 60, the adjusted death rate for the permanent residents would be maybe 8 times higher, or about 1.1%
The total number of positive cases for these ten countries are over 1.2 million, far more than any double blind test could ever produce.
Taking the average, adjusted for the number of positive cases, the average adjusted death rate for ten countries, where people are taking HCQ + Zinc as soon as they are showing symptoms or diagnosed positive, is 1.60%.
This means that the risk of death is reduced by a factor of 2.65 if HZQ + Zinc is taken as early as possible after showing symptoms or after a positive diagnosis for corona-virus!
This means the daily could be reduced by 3700 a day in the world if the HCQ regimen was implemented worldwide.
For the U.S.A. the number of deaths would be reduced by an average of over 400 a day at today’s case and death rates, if HZQ + Zinc is taken as early as possible after showing symptoms or after a positive diagnosis for corona-virus!
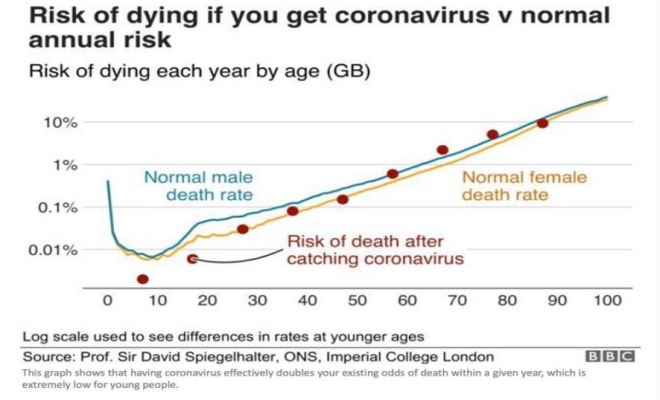
But wait. Not so fast. These countries have a younger population, and the death rate is much lower for younger people. This chart tells it all.
The death rate doubles for every 8 years as you age or about 9% per year. The world median age is 30.4 years. So let the world death rate be the norm
World death rate as of May 21 is 6.42% of diagnosed cases.
Turkey: Death rate 2.77%, median age 30.9, adjusted death rate 2.64%
South Korea: Death rate 2.37%, median age 30.9, adjusted death rate 2.26%
Malaysia: Death rate 1.61%, median age 28.5, adjusted death rate 1.91%
Senegal: Death rate 1.13%, median age 18.8, adjusted death rate 3.00%
Costa Rica: Death rate 1.11%, median age 31.3, adjusted death rate 1.02%
United Arab emirates: Death rate 0.88%, median age 30.9, adjusted death rate 0.84%
Bahrain: Death rate 1.43%, median age 32.3, adjusted death rate 1.20%
Morocco: Death rate 2.70%, median age 29.3, adjusted death rate 2.92%
Russia: Death rate 1.00%, median age 30.9, adjusted death rate 0.95%
Taking the average, not adjusted for the size of the populations we get the average adjusted death rate for countries, where people are taking HCQ + Zinc when diagnosed positive, is 1.89%.
This means that the risk of death is reduced by a factor of 3.4 if HZQ + Zinc is taken as early as possible after a positive diagnosis for coronavirus!
These 9 countries are living proof of it. Why are we not implementing it today?