Uttar Pradesh is India’s largest state with over 205 million people. It’s most famous shrine is the Taj Mahal.
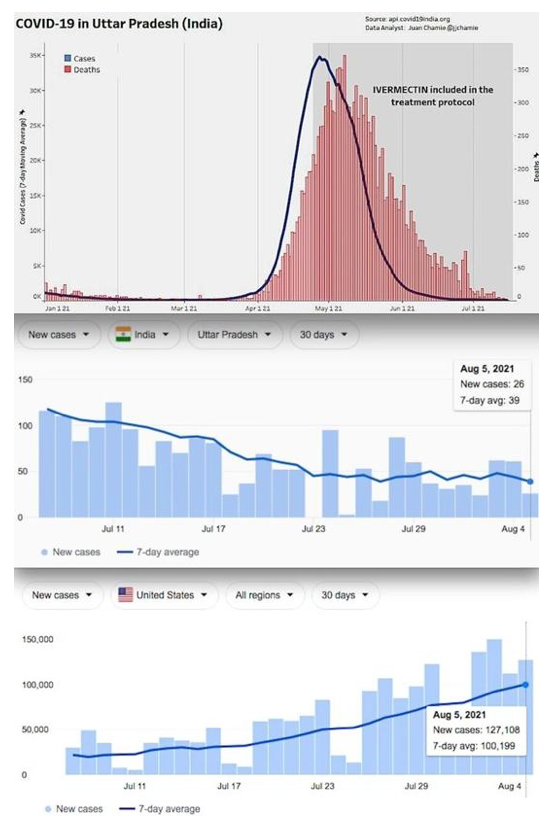
News of India’s defeat of the Delta variant should be common knowledge. It is just about as obvious as the nose on one’s face. It is so clear when one looks at the graphs that no one can deny it.
Yet, for some reason, we are not allowed to talk about it. Thus, for example, Wikipedia cannot mention the peer-reviewed meta-analyses by Dr. Tess Lawrie or Dr. Pierre Kory published in the American Journal of Therapeutics.
Wikipedia is not allowed to publish the recent meta-analysis on Ivermectin authored by Dr. Andrew Hill. Furthermore, it is not allowed to say anything concerning http://www.ivmmeta.com showing the 61 studies comprising 23,000 patients which reveal up to a 96% reduction in death [prophylaxis] with Ivermectin.
https://en.wikipedia.org/wiki/Talk%3AIvermectin
One can see the bias in Wikipedia by going on the “talk” pages for each subject and reading about the fierce attempts of editors to add these facts and the stone wall refusals by the “senior” editors who have an agenda. And that agenda is not loyalty to your health.
The easy way to read the “talk” page on any Wikipedia subject is to click the top left “talk” button. Anyone can then review the editors’ discussions.
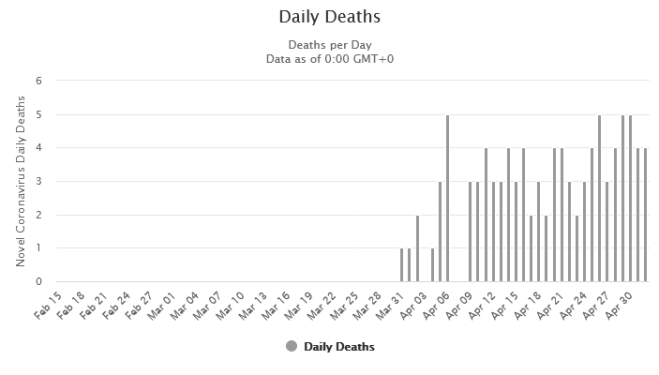
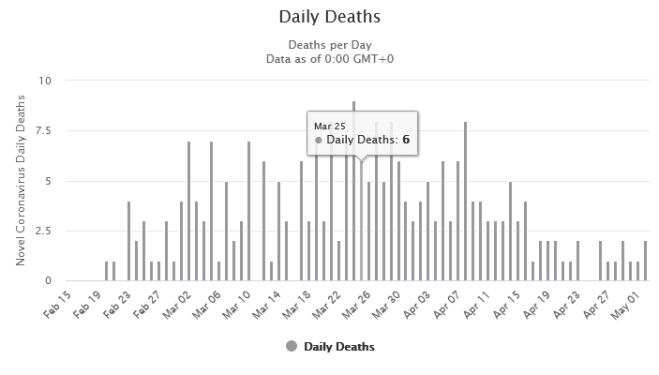
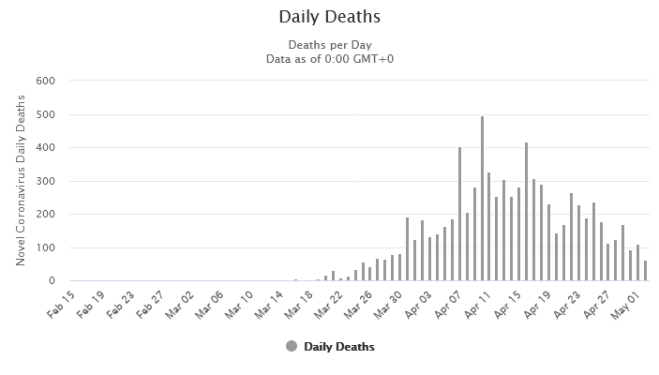
There is a blackout on any conversation about how Ivermectin beat COVID-19 in India. When I discussed the dire straits that India found itself in early this year with 414,000 cases per day, and over 4,000 deaths per day, and how that evaporated within five weeks of the addition of Ivermectin, I am often asked, “But why is there no mention of that in the news?”
Yes, exactly. Ask yourself why India’s success against the Delta variant with Ivermectin is such a closely guarded secret by the NIH and CDC. Second, ask yourself why no major media outlets reported this fact, but instead, tried to confuse you with false information by saying the deaths in India are 10 times greater than official reports.
Perhaps NPR is trying so hard because NPR is essentially a government mouthpiece. The US government is “all-in” with vaccines with the enthusiasm of a 17th century Catholic Church “all-in” with a Geocentric Model of the Universe disputing Galileo. Claiming that India’s numbers are inaccurate might distract from the overwhelming success of Ivermectin.
But in the end, the truth matters. It mattered in 1616, and it matters in 2021….
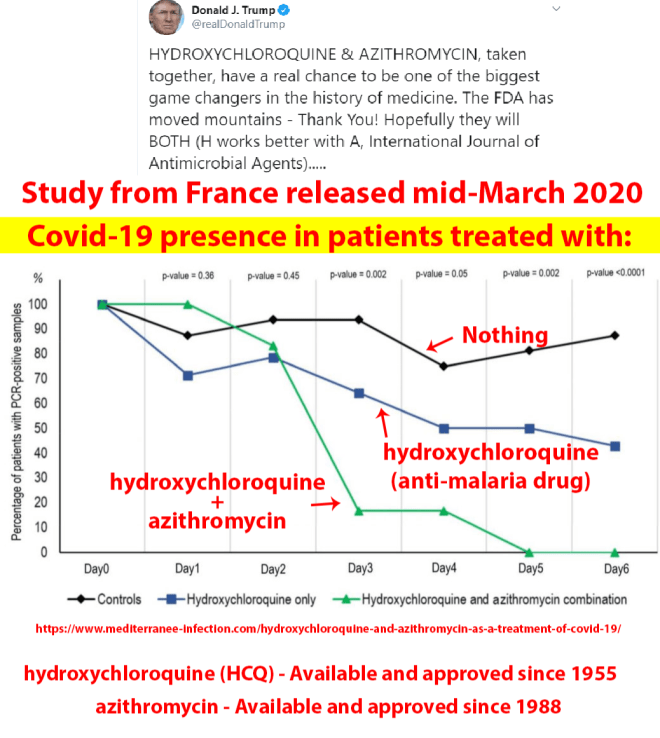
So, why are all media, CDC, NIH and the government all in on vaccines? This is my theory. When the Covid pandemic broke out, it was first downplayed by CDC, masks were not effective, just keep your distance and sanitize and it will go away. But it didn’t. In February, it was obvious that it was severe, and then President Trump suggested we develop a vaccine at warp speed, meaning in time for the election. Dr Fauci was conducting gain of function defense research at the Wuhan laboratory, so in less than a week, Pfizer and Moderna had a prototype vaccine ready for initial trials. Warp speed means, you test the vaccine as fast as possible, and at the same time promise to buy the vaccine by the hundreds of million doses, working or not. In March President Trump became a promoter of Hydroxychloroquine, and HCQ became a verboten subject. All clinical trials were stopped because of its danger, even though it had been approved for over 50 years against malaria, and used to control Lupus and some kinds of Rheumatisms. It is so safe that it is even used for pregnant women and nursing mothers. The countries that routinely used HCQ in the early stages had a much better disease outcome than countries that didn’t, but it was more important to get rid of Trump than to treat and cure the people. The vaccines are now here, approved for emergency use, and the death rate for people taking the vaccines is greater than could be expected for that age group, for children it is as high as a 60-fold increase. While data for COVID is abundant, the vaccine data is slow in coming. Then came Ivermectin, which is even more effective than HCQ, but it is not approved by CDC yet, even though it is approved for treatment of other diseases.
Then it hit me: The vaccines are for emergency use only, and can not be used if a cure is available. Since Vaccines are highly profitable and Ivermectin is cheap, the obvious decision for CDC is to not approve Ivermectin and ruin the vaccine revenue stream. The well being of the people is of no importance to CDC.
All other explanations are more sinister, so I refrain from further speculation.
In the Journal of Antibiotics a 12 June 2020 report on Ivermectin says: [https://www.nature.com/articles/s41429-020-0336-z]
“Several studies reported antiviral effects of ivermectin on RNA viruses such as Zika, dengue, yellow fever, West Nile, Hendra, Newcastle, Venezuelan equine encephalitis, chikungunya, Semliki Forest, Sindbis, Avian influenza A, Porcine Reproductive and Respiratory Syndrome, Human immunodeficiency virus type 1, and severe acute respiratory syndrome coronavirus 2.”
Professor Borody says his research has led him to a triple therapy of Ivermectin, zinc and an antibiotic – which are all TGA and FDA approved – which could be the fastest and safest way to stop the Victorian outbreak within 6-8 weeks. [See Professor Borody’s published research papers ORIC here http://orcid.org/0000-0002-0519-4698]
Professor Borody said, “These 3 medications are already approved. They do not need pre-clinical or clinical trials nor additional TGA approvals unless the aim is to combine in a single capsule, for example. Patient treatment programs have been done in the US and elsewhere which indicate it can work within 4-6 days.”
Professor Borody has reviewed the key antiviral scientific research literature and identified the combination of 3 drugs that are in chemists right now and can be prescribed by doctors immediately. The tablets can be taken at home as a preventive treatment by high risk individuals, or by those who test positive to minimise need for hospitalisation at the higher curative dose.
The therapy comprises:
- Ivermectin – TGA and FDA approved as an anti-parasitic therapy with an established safety profile since the 1970s. Known as the “Wonder Drug” from Japan.
- Zinc
- Doxycycline – TGA and FDA approved tetracycline antibiotic that fights infections, such as acne, urinary tract infections, intestinal infections, respiratory infections, eye infections, gonorrhea, chlamydia, syphilis, periodontitis (gum disease), and others.
Professor Borody says distribution teams could be deployed in Victoria’s hotspots to treat proven infected patients immediately, and people exposed or at risk could be taking the preventative dose.