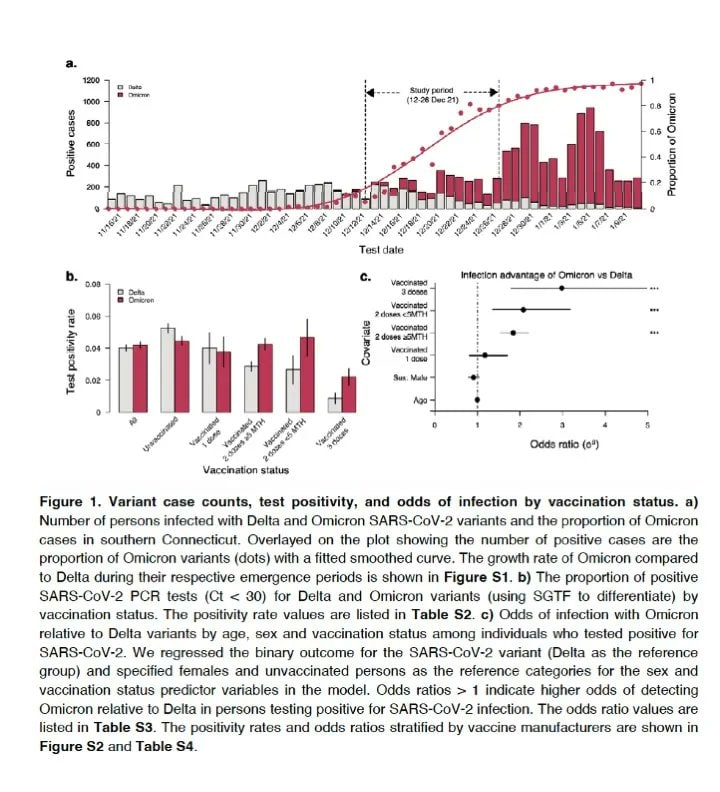
The take home from this pre-publication study is that there seems to be no difference in the probability of getting the Omicron variety of COVID or the Delta variety if you are unvaccinated, but the risk for being infected doubles if you are double vaccinated, and triple if you are also boosted. This means that the vaccines are less effective if you have had a booster shot for the Omicron variant. The Covid pandemic has moved from a pandemic of the unvaccinated to a pandemic of the vaccinated. My hopethesis is that the vaccines are too specific to work for a heavily mutated COVID such as the Omicron variety. We need a more broadband vaccine. Lucky for us they have changed the definition of what a vaccine is to include substances that lessen the impact of a disease, as prophylactic and therapeutic. With that definition there is already such a vaccine. It is called Ivermectin.
Let us test this hypothesis comparing the experience of U.S. and Nigeria. Since the start of the pandemic the U.S. has had 221,892 cases per million and 2,689 deaths per million people. By contrast, Nigeria has had 1,180 cases per million and 15 deaths per million, or about 0.53 percent of the cases and 1.27% of the deaths per million people.
How can that be? United states has the best medical system in the world, spending about 20% of GNP on medical care, Nigeria spends about 4% of their GNP on medical care. The median age for people in u.s is about 38.4 years, for Nigeria the median age is 18.4 years. The expected death risk for U.S.is about 5 times larger thanks to the age factor, so this makes up part of the difference. But the difference is far greater, so there must be something else. I am willing to accept that Nigeria has under-reported the number of cases, but the difference is much larger than can be explained this way. In addition Nigeria has one of the lowest vaccination rates in the world, less than 3%.
There is one better hypothesis, Nigeria has a great problem with River Blindness, a parasite on the skin that causes blindness if not treated. There is medication, given to all without cost, and it does the job. This medication is Ivermectin, and thanks to that the COVID cases are lower by a factor of 20, age-adjusted. Recently there has been a small study in Nigeria that seem to suggest that if you combine Ivermectin with HCQ and Zinc and Azithromycin, the results are even better. The results are presented here.
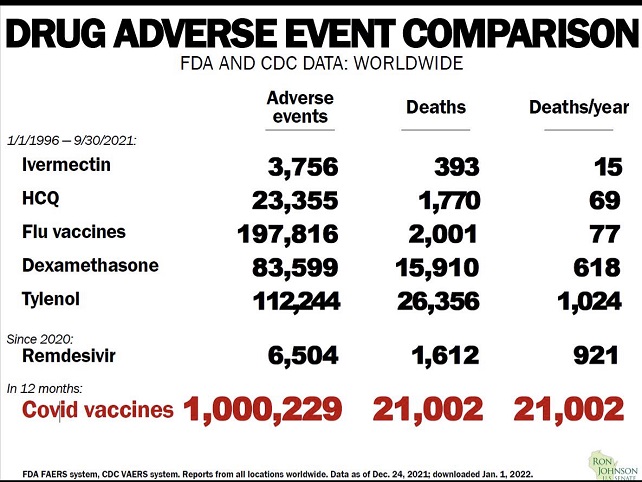
Want to save over a thousand deaths a day in U.S. alone? Switch immediately from vaccine only therapy to immediately allow Ivermectin and HydroxyChloroquine to be sold over the counter. The deaths from Ivermectin are only 15/ year worldwide and for Hydroxy Chloroquine 65/year worldwide, far less than say Tylenol, while the deaths from the vaccines are over 20,000 in the first year. The vaccines are great for people over 45, but for the younger generation the death risk outweighs the benefits.
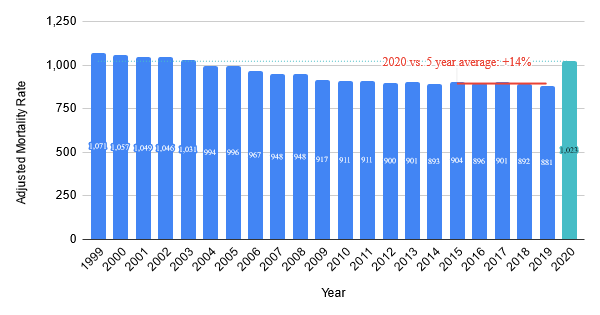
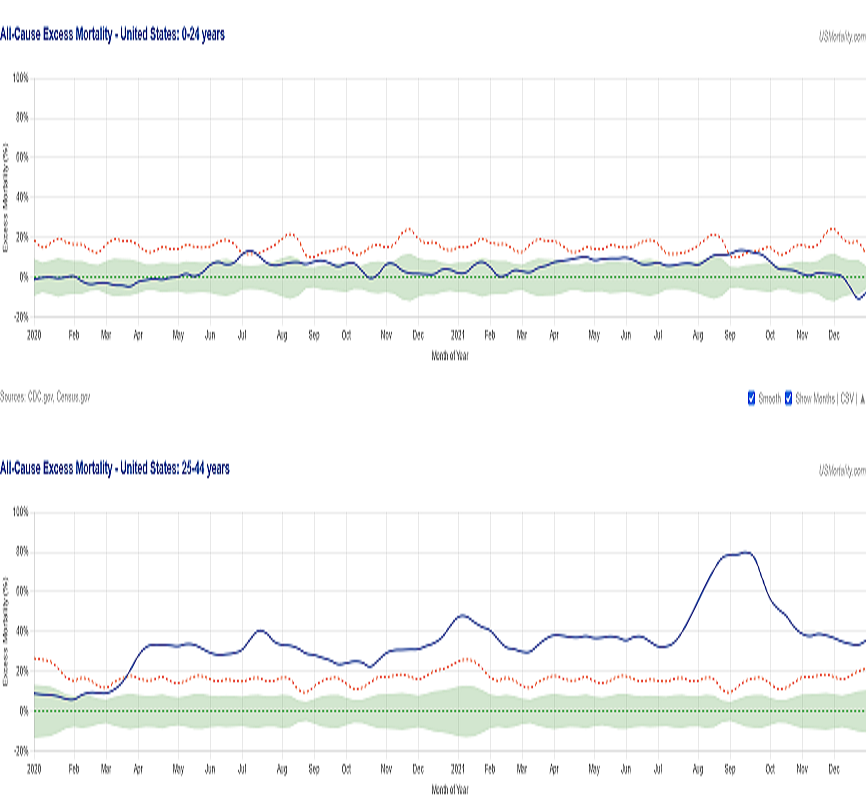
The U.s census is doing a remarkable job of statistics. This is from US Mortality
We can see the 2020 excess mortality was 14%Total 425,794 deaths broken down i 6 age categoriesPercentage wise it looks quite different!
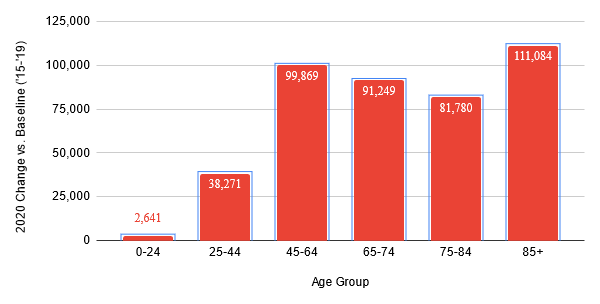
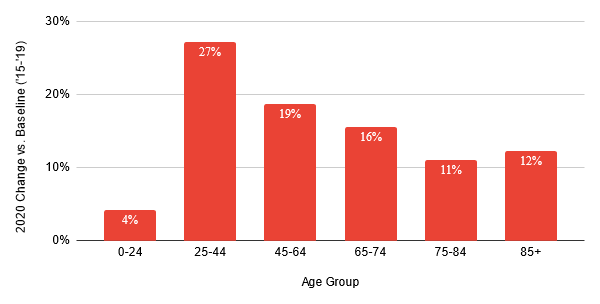
COVID deaths in 2020 was about 377,878 not much different than the total excess deaths. For the 6 categories they are as follow: 0-24 721 or 27% of excessive deaths; 25-44 9,144 or 24% of excessive deaths; 45-64 62,536 or 63% of excessive deaths; 65-74 80,617 or 88% of excessive deaths; 75-84 104,212 or 127% of excessive deaths; 85+ 120,648 or 109% of excessive deaths;
We can see that for people under 45 years of age only a quarter of the excess deaths came from COVID-19. Most of the deaths came from excess stress, delayed medical treatments, depression, drugs, drinking and misbehavior, but for people over 65 there was a positive effect of the protective provisions that followed. But 2020 was the year without vaccines and a learning year for how to best treat the pandemic.
So how are we doing in 2021? We now have three vaccines and have learnt a lot about how to best treat COVID. Well for openers COVID deaths in 2021 were 452 thousand, far more than in 2020! And we have learned a lot of best treatment for hospitalized patients. The official results are not in yet, but there are charts that can give us a clue.
The all cause excess mortality for the age group 0-24 years in 2021 is not much different than for 2020, the chart below indicate it is about 3% more, or about 4,000 excess deaths.
For the age group 25-44 years: From the time COVId started to the end of the year 2020 the excess mortality rate was about 30%. In 2021 the excess mortality ate was around 44%, or about 41,500 excess deaths.
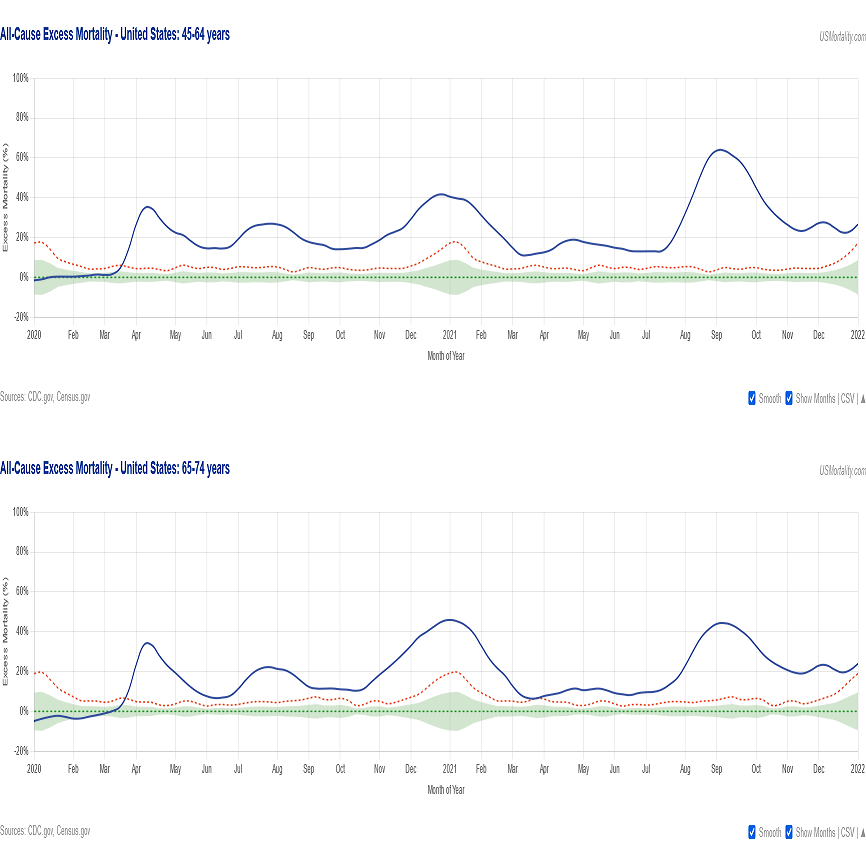
For the age group 45-64 years: From the time COVID started to the end of the year 2020 the excess mortality rate was about 23%. In 2021 the excess mortality ate was around 29%, or about 126,000 excess deaths.
For the age group 65-74 years: From the time COVID started to the end of the year 2020 the excess mortality rate was about 24%. In 2021 the excess mortality ate was around 22%, or about 84,000 excess deaths.
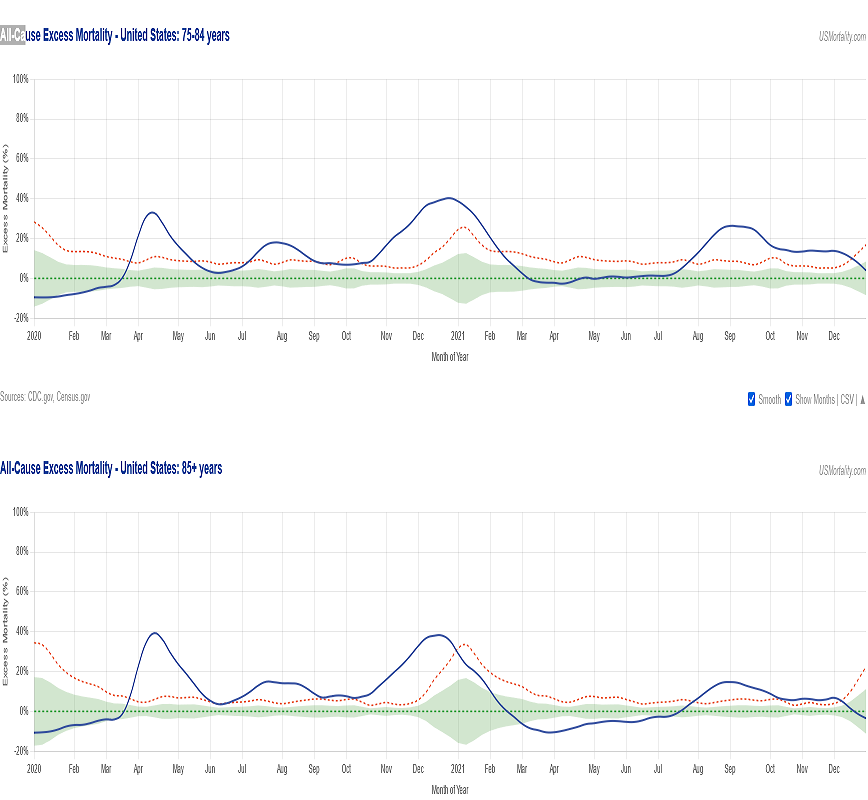
For the age group 75-84 years: From the time COVID started to the end of the year 2020 the excess mortality rate was about 18%. In 2021 the excess mortality ate was around 11%, or about 50,000 excess deaths.
And finally, for the age group 85+ years: From the time COVID started to the end of the year 2020 the excess mortality rate was about 18%. In 2021 the excess mortality ate was around 3%, or about 30,000 excess deaths.
First the good news. In 2020 the COVID-19 deaths were 89% of the total excessive deaths excessive deaths, in 2021 they were 131% of all excessive deaths. This means the vaccines are effective in reducing total deaths.
But do they reduce total deaths in all age categories?
For age group 0-24years: Excessive deaths 2020, 2,641 2021, 4,500, a 75% increase. 25-44years: Excessive deaths 2020, 38,271; 2021, 41,500, an 8.5% increase. 45-64years: Excessive deaths 2020, 99,869; 2021, 126,000, a 26% increase. 65-74years: Excessive deaths 2020, 91,249; 2021, 84.000, an 8% decrease. 75-84years: Excessive deaths 2020, 81,700; 2021, 50.000, a 39% decrease. 85+ years: Excessive deaths 2020, 111,284; 2021, 30.000, a 73% decrease.
Now, vaccines are not the only determining factor in the excessive deaths, overdoses of Fentanyl, opioids, alcohol and other drugs played a role. Especially in the 25-64 age group the additional stress to care for elderly parents while the children are still in high school or college plus being locked in at home and having to wear masks can be devastating to the mental health of anyone.
The conclusion from this study is: Dont vaccinate children and young adults. For people 25-44 vaccinate people with compelling medical needs to be protected. For people 45-64 make an informed decision, and since there are very often co-mprbidity factors, consider get vaccinated. For people over 65: By all means get vaccinated and boosted. Your immune system is already weakened anyway.
The vaccines that exist do not provide immunity. That was the old definition of vaccine. The new definition is that vaccines are prophylactic therapeutics for a time period, to be followed by boosters. There are two excellent prophylactic therapeutic medicines tha so fr has been overlooked by CDC, but are used at great advantage in much of the rest of the world: HydroxyChloroquine and Ivermectin. Check out Why is U.S.A. doing so poorly in fighting the pandemic? Is it beecause they refuse HCQ and Ivermectin?
It shows that the world has recorded 325,125,927 cases of the coronavirus and 5,550,676 deaths as of January 14 2022. U.S.A has recorded 66,250,206 cases and 872,332 deaths, or 20.4% of the world total cases but only 15.1% of the world’s deaths from the same virus. Great, we have more cases because we are doing more testing.
Not so, we have done 856 million tests, but the world has done over 4.8 billion tests, so our share of the testing is 17.8% or nearly the same as our part of the cases and deaths. But we are only 4.2% of the world population! This means we are doing three and a half times worse than the world as a total!
How can that be? We have the world’s best health care system with fantastic hospitals, full of state of the art equipment to monitor and do things that was unthinkable a decade ago. We are spending in excess of 10,000 dollars yearly per person on healthcare, while the global arithmetic average is less than 1200 dollars yearly per person, This means that most countries spend less than 1000 dollars yearly per person. In fact they are so poor that they cannot even think of spending for expensive patented medicines, so they are limited to the simplest generic prophylactic and therapeutic medicines. And you guessed it, they are mostly HydroxyChloroQuine and Ivermectin.
Why are we not approving Ivermectin and HCQ? They are ultra safe and they work. There are two reasons CDC is a vaccine approving agency and want dependent customers to purchase expensive medicines, and to approve Ivermectin and HCQ at this stage would mean that they would confess they have caused hundreds of thousand deaths by their refusal to approve them even they were far safer than say Remdesivir which was approved immediately after just one study (Hint it is expensive). We need to reorganize NIH, FDA and CDC to be patient oriented, no longer beholden to the medico-industrial behemoth.This is my opinion.
The headlines say it all. These are the results so far of adverse reactions to various medications and vaccines according to the official VAERS reporting, which give low estimates. The truth is worse. This is from Sen John Johnson:
It should be noted that for the first five medications the time frame is nearly 16 years, the result for COVID vaccine is one year.
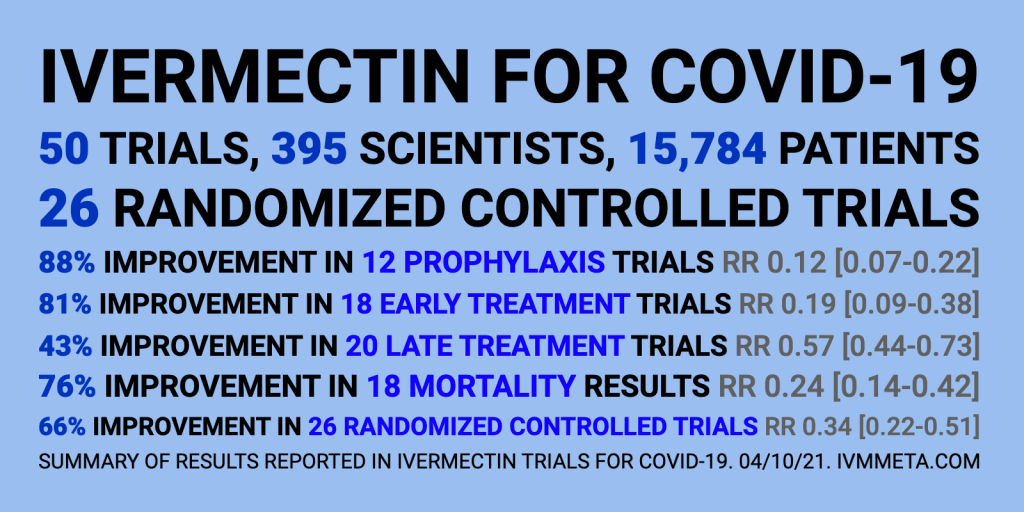
Of all medications that actually works against COVID with a more than 75% efficiency, Ivermectin has been approved for human use against river blindness and other parasites, such as head lice since late 1980’s. The countries in Africa that routinely use it for parasite control have a COVID case and death rate of less than 1/10th of the countries in Africa that don’t. There are almost no adverse reactions.
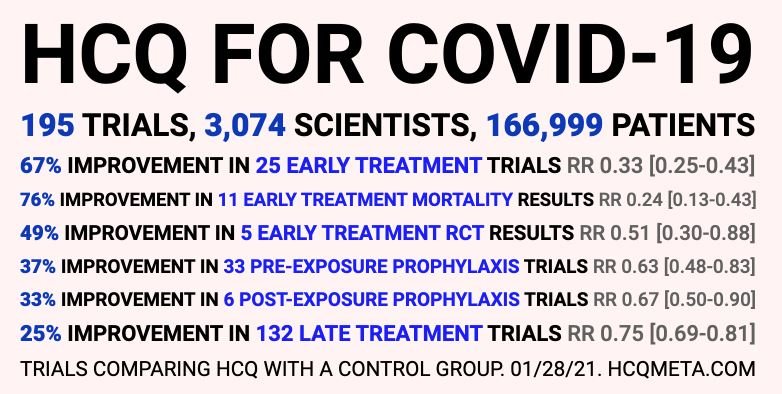
HCQ is almost as good COVID fighter as Ivermectin when taken early in conjunction with Zinc. It’s effectiveness is at least 65% and has been used for over 50 years as an anti malaria drug, against lupus and some rheumatoid diseases. It is given to pregnant women and nursing mothers without restrictions.
Flue vaccines have very few adverse effects, but they happen.
Remdisivir was approved very fast, after all, it was expensive and showed early promising results, but it turned out that nearly 30% of the test clientele had used HCQ before entering the protocol. It turned out, that without HCQ it was not so good after all.
Alone in the history of vaccines has COVID vaccines been approved with such a staggering rate of adverse reactions and over 20,000 deaths from the vaccine in a year. Yet it helps people at risk, people over 60, obese, diabetic, anemic, vitamin C and D deficiency, immune compromised, high blood pressure and a variety of diseases, so they were important in the beginning of the disease, and will be for a while until the therapeutics are approved.
In the mean time , children and young adults without additional risk factors are at higher risk of dying if they take the vaccine than if they get COVID, older people should still go the vaccine route. With admittedly limited statistics available I have calculated the crossover point to be 45 years for people without additional risk factors.
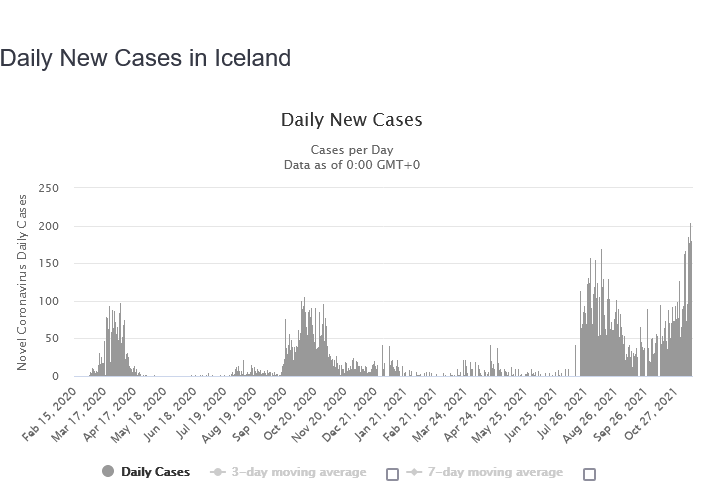
Icealand is a unique country with active volcanoes, Geysers, hot springs and glaciers. It has also one the highest vaccination rates in the world; 83 % of the whole population has received at least one dose by Nov 13, and 81.0 percent are fully vaccinated. Already early June over 50% of the population had received at least one dose of vaccination; so they are now six months into what can be called fully vaccinated, since 7.8% of the population are not eligible, being children under 12 years of age.
How are they doing?
Iceland was doing remarkably well until May of 2021, when most people got their doses of vaccine, and cases fell to near zero during June and July, which “proved” the efficacy of the vaccine until August when cases suddenly rose again and were on Nov 11 more than twice as many as the highest daily total before vaccinations began.
It turns out that the vaccine they have received is not a vaccine in the old definition of vaccine, something that grants immunity to the disease, so CDC has changed the definition of vaccine to mean something that lessens the symptoms of the disease. So all vaccinated people have now the capacity to become “typhoid Marys” keeping reinfecting each other, both vaccinated and unvaccinated.
Are Icelanders allowed to take Ivermectin against COVID-19? Probably not. One person was hospitalized using Soolandra a skin care product whose active ingridient is 1% Ivermectin. He ingested an unknown amount and the medical community sent out a warning against using Soolantra even though the warning to not ingest it is right on the package. People get desperate when Ivermectin is forbidden in tablet form, they even swallow horsepaste Ivermectin even though the formulation for horses is quite different from the tablet form for people.
The good news is that even though infection rates have skyrocketed, deaths rates have fallen.
I am still of the opinion that it is better to cure the disease using HydroxyChloroQuine or Ivermectin together with Zinc and an anti inflammatory drug and thus control the disease than having to take booster shots for ever and remain “Typhoid Marys”.
In Indiatoday Prabhash K Dutta, New Delhi wrote in June 7, 2021:
Remember Donald Trump-touted hydroxychloroquine? Study in India backs it as Covid-19 cure.
Hydroxychloroquine, the malaria drug touted as a magical Covid-19 cure by former US President Donald Trump last year, has been found effective in a prophylactic study published in a prophylactic study published in the Journal of The Association of Physicians of India (JAPI)
The study showed that hydroxychloroquine, popularly known as HCQ, could prevent SARS-CoV-2 infection in varying degrees depending on its dosing regimen. The highest prevention rate of 72 per cent was found among those given hydroxychloroquine over six weeks or a longer duration.
The study said, “[W]hen adjusted for other risk factors, HCQ dose as per government recommendations, 2-3, 4-5, 6 or more weeks reduced the probability of Covid positivity by 34 per cent, 48 per cent and 72 per cent.”
The study was conducted May-September last year when HCQ was still part of the Union health ministry’s recommendation in treatment protocol for Covid-19, and it began against the backdrop of contesting claims made by authorities and experts including Donald Trump and his advisor Dr Anthony Fauci, the US’s top infectious disease expert.
In March 2020, Donald Trump declared that hydroxichloroquine was a “game changer” drug in the fight against Covid-19. Dr Fauci dismissed the claim citing lack of study and evidence. Despite Fauci’s counter-positioning, Trump continued to be vocal about taking HCQ as prophylactic drug.
Incidentally, the Union health ministry on June 6 dropped hydroxychloroquine from Covid-19 treatment protocol. In its nine-page guidelines released on Sunday (June 6) by the directorate of health services, hydroxychloroquine, ivermectin and favipiravir find no mention.
The government’s decision came on the back of criticism by experts who pointed out a lack of study-based evidence to recommend hydroxychloroquine in Covid-19 cases. The government’s revised guidelines, however, contradicts the recommendations made by the Indian Council of Medical Research as released on May 17.
The ICMR guidelines prescribed the use of hydroxychloroquine in mild cases of Covid-19.
The authors of this prophylactic (relating to prevention of a disease) study said that this “is the largest multicenter study on HCQ prophylaxis on HCWs (healthcare workers), covering over 12,000 HCWs at the risk of Covid-19”.
The study was conducted in May-September last year across 44 hospitals in 17 states involving hundreds of doctors, who received doses of hydroxychloroquine.
One of the co-authors of the study, Dr Raj Kamal Choudhry said, “In the 1985-86 edition of Harrison’s Principles of Internal Medicine [a highly recommended book for students studying medicine in medical colleges], Dr. Fauci wrote that HCQ worked an anti-viral agent despite being an anti-malarial drug. There was no Covid-19 back then, but HCQ’s anti-viral properties were already well known.”
Dr Raj Kamal Choudhry, who was the nodal officer for the prophylaxis study of HCQ in Bihar’s Bhagalpur medical college, said, “We had given about 2,700 doctors and paramedical staff, laundry and kitchen people the prophylaxis of HCQs in the dose of HCQs 400 mg 1×2 for first day then 1 tab daily for 4 days.”
“We did not give to those who had palpitations and had QT prolongation [a measure of heart ailment]. Those who took this drug did not have Covid excepting 5 and 6. The effect was tremendous. Later, we gave this drug to all who had mild cases. Only those patients who were in ICU were not given.”
“Of 2,700 people who were given HCQs, 700 were doctors. Only five or six got infected with SARS-CoV-2 in Bhagalpur but none developed serious complications, and nobody died of Covid-19,” Dr Raj Kamal Choudhry told Indiatoday.in.
The evidence is piling up. There has been numerous, over 50 studies like this showing that HCQ is effective, both as prophylactic, and as an early cure. Yoo bad that the medical bureaucracy considered it more important to get rid of Donald Trump than to save over 100,000 lives in U.S. alone.
In addition HCQ is too cheap and generic to warrant a double blind study.
The other medication that may be as effective, and save lives is Ivermectin, an anti-parasite drug used to treat horses and other farm animals. You can buy it at Tractor Supply, so I have been told.
The chairman of the Tokyo Medical Association, Haruo Ozaki, held a press conference August 13, announcing that the anti-parasite medicine Ivermectin seems to be effective at stopping COVID-19 and publicly recommending that all doctors in Japan immediately begin using Ivermectin to treat COVID.
“Several studies reported antiviral effects of ivermectin on RNA viruses such as Zika, dengue, yellow fever, West Nile, Hendra, Newcastle, Venezuelan equine encephalitis, chikungunya, Semliki Forest, Sindbis, Avian influenza A, Porcine Reproductive and Respiratory Syndrome, Human immunodeficiency virus type 1, and severe acute respiratory syndrome coronavirus 2.”
Professor Borody says his research has led him to a triple therapy of Ivermectin, zinc and an antibiotic – which are all TGA and FDA approved – which could be the fastest and safest way to stop the Victorian outbreak within 6-8 weeks. [See Professor Borody’s published research papers ORIC here http://orcid.org/0000-0002-0519-4698]
Professor Borody said, “These 3 medications are already approved. They do not need pre-clinical or clinical trials nor additional TGA approvals unless the aim is to combine in a single capsule, for example. Patient treatment programs have been done in the US and elsewhere which indicate it can work within 4-6 days.”
Professor Borody has reviewed the key antiviral scientific research literature and identified the combination of 3 drugs that are in chemists right now and can be prescribed by doctors immediately. The tablets can be taken at home as a preventive treatment by high risk individuals, or by those who test positive to minimise need for hospitalisation at the higher curative dose.
The therapy comprises:
Ivermectin – TGA and FDA approved as an anti-parasitic therapy with an established safety profile since the 1970s. Known as the “Wonder Drug” from Japan.
Zinc
Doxycycline – TGA and FDA approved tetracycline antibiotic that fights infections, such as acne, urinary tract infections, intestinal infections, respiratory infections, eye infections, gonorrhea, chlamydia, syphilis, periodontitis (gum disease), and others.
Professor Borody says distribution teams could be deployed in Victoria’s hotspots to treat proven infected patients immediately, and people exposed or at risk could be taking the preventative dose.
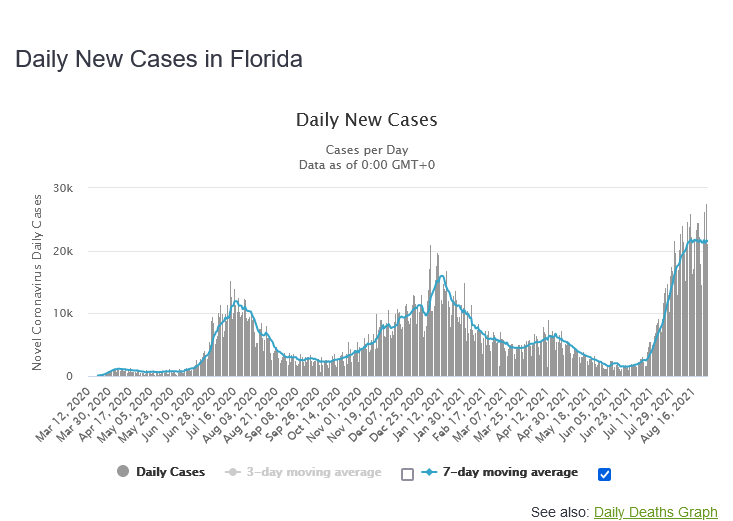
The Governor of Florida, DeSantis is promoting the use of Regeneron. Florida has one of the highest outbreaks of the Delta variant of the Covid-19 virus.
What is Regeneron?
Regeneron, which is being used at all Florida sites, is a common name for REGEN-COV, a monoclonal antibody treatment manufactured by Regeneron Pharmaceuticals.
“It’s the only monoclonal that’s had success against the delta variant,” DeSantis said, adding another benefit is the injections take only minutes instead of an IV that takes an hour. But there is a short window of opportunity.
“You’ve got to do this early, so if you are infected, by the time you get very, very ill and require hospitalization, it’s probably too late for this to work,” he said. “Clearly, the sooner you do it, the better you’re going to be.”
Studies have shown a 70% reduction in hospitalizations among people who have had a monoclonal antibody treatment, DeSantis said.
The treatment isn’t for everyone; REGEN-COV is “an unapproved investigational therapy, and there are limited clinical data available,” the drug’s website cautions.
REGEN-COV is not authorized to treat coronavirus patients who are hospitalized or require oxygen therapy. Citing insufficient data, the manufacturer recommends pregnant women receive the drug only when the benefits outweigh the risks for mother and child.
“Anyone I talked to who had gotten the Regeneron had positive things to say about it,” DeSantis said. “They would just say, ‘I felt so bad, then all of a sudden, I took it and 24 to 48 hours later, I felt much better, my symptoms were resolved.’ You hear that over and over again, and we are hearing it with a lot of the patients that are coming through our sites.”
How are the results so far? See the cases rise and deaths decrease for Florida and judge for yourselves:
Cases as of August 28: 214897 day average for deaths as of August 28: 68.
As we can see, deaths plummeted when Regeneron treatment became widely used on seriously ill patients, and the death rate is now 0.32%, going lower.
One more thing, make sure you take supplemental Vitamin D3 (I take 5000 IU/day). An Indonesian study found that the death rate went from 95% if the values were less than 19 nanograms/milliliter to less than 5% if the D3 values were over 31 nanograms/milliliter. The study was made in Covid patients over 65 years old.
Who should get vaccinated? For me, being nearly 80 years old, with a heart condition and a severe blood disease the choice was easy. Of course, I should get vaccinated. But for younger people, people under 45 years of age with a more than 99.9% chance of survival even without HCQ, Ivermectin or Regeneron treatment should they get the Covid.
NEW BLOOMFIELD — A Cleveland Clinic study released this week stated people already infected with the coronavirus gain no additional benefits from vaccination.
The study included 52,000 Cleveland Clinic employees and found not one person who was infected with the virus and chose not to get vaccinated became reinfected.
The data led researchers to conclude those already infected with COVID-19 gain no benefit from getting the vaccine, but an MU Health Care official disagrees with the clinic’s statement.
With this new information my recommendation is to only perform vaccination on demand to preserve personal freedom as much as possible, recommend it to high risk groups, but do not vaccinate children and college age adults! We are close enough to herd immunity to carry out the vaccine trials and prove them effective and safe for the long run before we proceed any further. After all, the vaccines are only approved for emergency use, and children and young adults do not die from it, but the side effects of the vaccine are often much more severe than the disease itself. In children it is mostly asymptomatic. For young adults there is a disturbing rise in the myocarditis after taking the vaccine.
This was in 2005. Dr. Fauci knew then HydroxyChloroQuine was effective against Covid type viruses. “In the 1985-86 edition of Harrison’s Principles of Internal Medicine [a highly recommended book for students studying medicine in medical colleges], Dr. Fauci wrote that HCQ worked an anti-viral agent despite being an anti-malarial drug. There was no Covid-19 back then, but HCQ’s anti-viral properties were already well known.
In 2015 the only level-4 virus lab in the U.S. conducting defensive research against “Gain of function” viruses was closed because of the inherent danger to the population should the virus escape. Not to worry, President Obama, Melinda Gates and Dr Fauci started to look for a new place to conduct the research. They found it in Wuhan, China; the Chinese have no such scruples as danger to the people. This lab was taken over in 2017 by the Chinese army, conducting bio-weapon research (defensive only, of course), so the research continued, this time controlled by the Chinese.
In January 2017 Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, said there is “no doubt” Donald J. Trump will be confronted with a surprise infectious disease outbreak during his presidency.
It is getting interesting. The virus escaped the lab, sometimes in the fall of 2019, and the Chinese knew it but kept silent. They closed off Wuhan to all other Chinese, rail, car and air. But they kept international travel open, as if they wanted the virus to spread all around the world. And Dr. Fauci knew it!
In Indiatoday Prabhash K Dutta, New Delhi wrote in June 7, 2021:
Remember Donald Trump-touted hydroxychloroquine? Study in India backs it as Covid-19 cure.
Hydroxychloroquine, the malaria drug touted as a magical Covid-19 cure by former US President Donald Trump last year, has been found effective in a prophylactic study published in a prophylactic study published in the Journal of The Association of Physicians of India (JAPI) last week..
The study showed that hydroxychloroquine, popularly known as HCQ, could prevent SARS-CoV-2 infection in varying degrees depending on its dosing regimen. The highest prevention rate of 72 per cent was found among those given hydroxychloroquine over six weeks or a longer duration.
The study said, “[W]hen adjusted for other risk factors, HCQ dose as per government recommendations, 2-3, 4-5, 6 or more weeks reduced the probability of Covid positivity by 34 per cent, 48 per cent and 72 per cent.”
The study was conducted May-September last year when HCQ was still part of the Union health ministry’s recommendation in treatment protocol for Covid-19, and it began against the backdrop of contesting claims made by authorities and experts including Donald Trump and his advisor Dr Anthony Fauci, the US’s top infectious disease expert.
In March 2020, Donald Trump declared that hydroxichloroquine was a “game changer” drug in the fight against Covid-19. Dr Fauci dismissed the claim citing lack of study and evidence. Despite Fauci’s counter-positioning, Trump continued to be vocal about taking HCQ as prophylactic drug.
Incidentally, the Union health ministry on June 6 dropped hydroxychloroquine from Covid-19 treatment protocol. In its nine-page guidelines released on Sunday (June 6) by the directorate of health services, hydroxychloroquine, ivermectin and favipiravir find no mention.
The government’s decision came on the back of criticism by experts who pointed out a lack of study-based evidence to recommend hydroxychloroquine in Covid-19 cases. The government’s revised guidelines, however, contradicts the recommendations made by the Indian Council of Medical Research as released on May 17.
The ICMR guidelines prescribed the use of hydroxychloroquine in mild cases of Covid-19.
The authors of this prophylactic (relating to prevention of a disease) study said that this “is the largest multicenter study on HCQ prophylaxis on HCWs (healthcare workers), covering over 12,000 HCWs at the risk of Covid-19”.
The study was conducted in May-September last year across 44 hospitals in 17 states involving hundreds of doctors, who received doses of hydroxychloroquine.
One of the co-authors of the study, Dr Raj Kamal Choudhry said, “In the 1985-86 edition of Harrison’s Principles of Internal Medicine [a highly recommended book for students studying medicine in medical colleges], Dr. Fauci wrote that HCQ worked an anti-viral agent despite being an anti-malarial drug. There was no Covid-19 back then, but HCQ’s anti-viral properties were already well known.”
Dr Raj Kamal Choudhry, who was the nodal officer for the prophylaxis study of HCQ in Bihar’s Bhagalpur medical college, said, “We had given about 2,700 doctors and paramedical staff, laundry and kitchen people the prophylaxis of HCQs in the dose of HCQs 400 mg 1×2 for first day then 1 tab daily for 4 days.”
“We did not give to those who had palpitations and had QT prolongation [a measure of heart ailment]. Those who took this drug did not have Covid excepting 5 and 6. The effect was tremendous. Later, we gave this drug to all who had mild cases. Only those patients who were in ICU were not given.”
“Of 2,700 people who were given HCQs, 700 were doctors. Only five or six got infected with SARS-CoV-2 in Bhagalpur but none developed serious complications, and nobody died of Covid-19,” Dr Raj Kamal Choudhry told Indiatoday.in.
The evidence is piling up. There has been numerous, over 50 studies like this showing that HCQ is effective, both as prophylactic, and as an early cure. Yoo bad that the medical bureaucracy considered it more important to get rid of Donald Trump than to save over 100,000 lives in U.S. alone.
In addition HCQ is too cheap and generic to warrant a double blind study.
The other medication that may be as effective, and save lives is Ivermectin, an anti-parasite drug used to treat horses and other farm animals. You can buy it at Tractor Supply, so I have been told. I do not know proper dosages, but if done properly, it is safe for humans when treating parasitic infections. It also is too cheap for the medical community to take seriously.
One more thing, make sure you take supplemental Vitamin D3 (I take 5000 IU/day). An Indonesian study found that the death rate went from 95% if the values were less than 19 nanograms/milliliter to less than 5% if the D3 values were over 31 nanograms/milliliter. The study was made in Covid patients over 65 years old.
I have counted the u.s covid-19 cases cases and deaths for the first week of April, and divided them by states requiring mask wearing and not requiring wearing masks. The mask wearing states had a death rate of 0.91% while the non mask wearing states had a death rate of 1.59%. The non mask wearing states had 244 deaths per day. This means we could have saved 244 (1.59-0,91)/1.59 = 103 lives per day as a nation if all were forced to wear a mask, everything else being equal (which of course it isn’t). (Look at Appendix 1 to see how your state is faring.)
Are there any better ways to save lives?
In March 2020 President Trump became a proponent of using HydroxyChloroQuine as a remedy for Covid-19. It was met with strong opposition from CDC and even scorn from his political opponents. CDC even published strong advice against using it to treat Covid-19, while still recommending its use to treat Lupus and rheumatoid patients with essentially no restrictions, including pregnant women and nursing mothers. After all, it had an over 50 year safety record as treatment for Malaria. Even Dr Fauci acknowledged its safety and efficacy as a cure for Coronaviruses as early as 2005, (see Appendix 2). Many countries are using HCQ as a first defense against COVID-19, and they experience on average less than half the death rate of nations that do not use HCQ as a first defense. To complicate matters, HCQ is prescribed to between 16 and 30% of all Covid cases in the U.S. As a guess with today’s 491 death’s per day, we could have saved more than 40%, about 200 lives a day, or twice as many lives as are saved by the mask mandate. The biggest problem for CDC is that HCQ is generic, cheap and easy to produce, so there is no profit in making a double blind study. For Trump opponents it was far more important to defeat Trump than to save a hunded thousand lives. ( see https://lenbilen.com/2020/09/06/u-s-a-corona-virus-death-rate-as-of-september-5-is-3-00-41-countries-have-higher-death-rates-15-countries-giving-hcqzincz-pac-to-covid-19-patients-as-soon-as-symptoms-occur-have-much-lower-death/ )
But there are other interesting cures for COVID-19, Ivermectin is fantastic. It has one problem, through.You can buy it at Tractor-supply, it is used as an antiparasitic agent for dogs and horses, and it is generic. However the worldwide interest is so big that at least 50 trials have been conducted and there is a 76% decrease in mortality. That means,using it properly would save nearly 400 lives per day.
This article needs wide distribution. It is eye-opening, showing clearly the Chinese origin and intent with the China-virus. It also shows the difficulty in developing a universal vaccine against it; it may never succeed. This means we may have to live through the pandemic until herd immunity is established, like Sweden has been doing. The solution is to concentrate on therapeutics, and the .minimum we should do is to immediately release the HCQ + Z-max + Zinc remedy for sale over the counter. Here is a petition to the WhiteHouse to allow HCQ to be sold over the counter. Please sign it if you are concerned about saving lives. According to the Ford study treatment with hydroxychloroquine cut the death rate significantly in sick patients hospitalized with COVID-19 – and without heart-related side-effects, according to a new study published by Henry Ford Health System. The death rate was cut in half for patients treated with HCQ. It it even more dramatic if HCQ is administered as soon as symptoms occur, over 40 international studies have shown an up to 80+% reduction in death rates. For some reason FDA and CDC do not acknowledge international studies.
The article:
August 10, 2020 (LifeSiteNews) author: Stephen Mosher – It will not be possible for the Dr. Fauci’s of the world to dismiss Professor Giuseppe Tritto as a crank. Not only is he an internationally known expert in biotechnology and nanotechnology who has had a stellar academic career, but he is also the president of the World Academy of Biomedical Sciences and Technologies (WABT), an institution founded under the aegis of UNESCO in 1997.
In other words, he is a man of considerable stature in the global scientific community. Equally important, one of the goals of WABT is to analyze the effect of biotechnologies—like genetic engineering—on humanity.
In his new book, this world-class scientist does exactly that. And what he says is that the China Virus definitely wasn’t a freak of nature that happened to cross the species barrier from bat to man. It was genetically engineered in the Wuhan Institute of Virology’s P4 (high-containment) lab in a program supervised by the Chinese military.
Prof. Tritto’s book, which at present is available only in Italian, is called Cina COVID 19: La Chimera che ha cambiato il Mondo(China COVID 19: The chimera that changed the world). It was published on August 4 by a major Italian press, Edizioni Cantagalli, which coincidently also published the Italian edition of one of Stephen Mosher’s books, Population Control (Controllo Demografico in Italian) several years ago.
What sets Prof. Tritto’s book apart is the fact that it demonstrates—conclusively, in Stephen Mosher’s view—the pathway by which a PLA-owned coronavirus was genetically modified to become the China Virus now ravaging the world. His account leaves no doubt that it is a “chimera”, an organism created in a lab.
He also connects the dots linking the Wuhan lab to France and the United States, showing how both countries provided financial and scientific help to the Chinese as they began to conduct ever more dangerous bioengineering experiments. Although neither American nor French virologists are responsible for the end result—a highly infectious coronavirus and a global pandemic—their early involvement may explain why so many insist that the “chimera” must have come from nature. The last thing they want to admit is that they might have had a hand in it.
In 2015 President Barack Obama, Dr. Anthony Fauci and Melinda Gates visited the Wuhan lab after giving a 3.5 million research grant to study bat viruses and maybe develop a vaccine against it. At some other forum he also said ” there is “no doubt” Donald J. Trump will be confronted with a surprise infectious disease outbreak during his presidency.”
Those of us who, early on, argued for a laboratory origin were dismissed as conspiracy theorists. Our articles were censored as “fake news,” often by American virologists who knew perfectly well what the truth was, but preferred to protect China, and themselves, from scrutiny lest they themselves be implicated.
Dr. Tritto’s 272 pages of names, dates, places, and facts leaves such apologists with no place to hide. The story begins following the SARS epidemic of 2003, as the Chinese attempt to develop vaccines to combat the deadly disease. Dr. Shi Zhengli, about whom I have previously written, was in charge of the program at the Wuhan Institute of Virology.
In vaccine development, reverse genetics is used to create viral strains that have reduced pathogenicity but to which the immune system responds by creating antibodies against the virus. But reverse genetics can also be used to create viral strains that have increased pathogenicity. That is what Dr. Shi, encouraged by PLA bioweapons experts, began increasingly to focus her research on, according to Prof. Tritto.
Dr. Shi first solicited help from the French government, which built the P4 lab, and from the country’s Pasteur institute, which showed her how to manipulate HIV genomes. The gene insertion method used is called “reverse genetics system 2.” Using this method, she inserted an HIV segment into a coronavirus discovered in horseshoe bats to make it more infectious and lethal.
The U.S. was involved as well, particularly Prof Ralph S. Baric, of the University of North Carolina, who was on the receiving end of major grants from the National Institute of Allergy and Infectious Disease. This is, of course, Dr. Anthony Fauci’s shop. Fauci was a big proponent of “gain of function” research, and when this was prohibited at Baric’s lab because it was considered to be too dangerous, the research was shifted to China.
Prof. Tritto believes that, while Dr. Shi’s research began as an effort to develop a vaccine against SARS, it gradually morphed into an effort to use “reverse genetics” to build lethal biological weapons. This was the reason that the Wuhan lab became China’s leading center for virology research in recent years, attracting major funding and support from the central government.
Stephen Mosher would add that the rule in Communist-controlled China is “let the civilian support the military,” which means that as soon as Dr. Shi’s research showed any potential military uses the PLA would have begun exercising control of the research. This came out in the open with the outbreak, when China’s leading expert on bioweapons, People’s Liberation Army Major General Chen Wei, was immediately placed in charge of the Wuhan Institute of Virology. As for Dr. Shi Zheng-Li, she seems to have disappeared.
As Dr. Tritto explained in an interview with Italian media:
In 2005, after the SARS epidemic, the Wuhan Institute of Virology was born, headed by Dr. Shi Zheng-Li, who collects coronaviruses from certain bat species and recombines them with other viral components in order to create vaccines. In 2010 she came into contact with American researchers led by Prof. Ralph Baric, who in turn works on recombinant viruses based on coronaviruses. Thanks to the matrix viruses provided by Shi, Baric created in 2015 a mouse Sars-virus chimera, which has a pathogenic effect on human cells analyzed in vitro.
At that point, the China-US collaboration becomes competition. Shi wants to work on a more powerful virus to make a more powerful vaccine: it combines a bat virus with a pangolin virus in vitro and in 2017 publishes the results of this research in some scientific articles.
Her research attracts the interest of the Chinese military and medical-biological sector which deals with biological weapons used as a deterrent for defensive and offensive purposes. Thus Shi is joined by doctors and biologists who belong to the political-military sphere, such as Guo Deyin, a scholar of anti-AIDS and anti-viral hepatitis vaccines and expert in genetic recombination techniques. The introduction of the new engineered inserts into the virus genome is the result of the collaboration between the Shi team and that of Guo Deyin. The realization of this new chimera, from a scientific point of view, is a success. So much so that, once the epidemic has broken out, the two researchers ask WHO to register it as a new virus, H-nCoV-19 (Human new Covid 19), and not as another virus derived from SARS. It is reasonable to think that Shi acted only from the point of view of scientific prestige, without however taking into account the risks in terms of security and the political-military interests that her research would have aroused.
When asked why China has refused to provide the complete genome of the China Virus to the WHO or to other countries, Dr. Tritto explained that “providing the matrix virus would have meant admitting that SARS-CoV-2 [China Virus] was created in the laboratory. In fact, the incomplete genome made available by China lacks some inserts of AIDS amino acids, which itself is a smoking gun.”
The key question, for those of us who are living through the pandemic, concerns the development of a vaccine. On this score, Prof. Tritto is not optimistic:
Given the many mutations of SARS-CoV-2, it is extremely unlikely that a single vaccine that blocks the virus will be found. At the moment 11 different strains have been identified: the A2a genetic line which developed in Europe and the B1 genetic line which took root in North America are more contagious than the 0 strain originating in Wuhan. I therefore believe that, at the most, a multivalent vaccine can be found effective on 4-5 strains and thus able to cover 70-75% of the world’s population.
In other words, by withholding from the world the original genetic code of the China Virus that it created, the Chinese Communist Party is ensuring that no completely effective vaccine will ever be developed by the West.
In other words, China continues to lie, and people continue to die.
Steven W. Mosher @StevenWMosher is the President of the Population Research Institute and the author of Bully of Asia: Why China’s “Dream” is the New Threat to World Order.




 August 10, 2020 (
August 10, 2020 (