In Indiatoday Prabhash K Dutta, New Delhi wrote in June 7, 2021:
Remember Donald Trump-touted hydroxychloroquine? Study in India backs it as Covid-19 cure.
Hydroxychloroquine, the malaria drug touted as a magical Covid-19 cure by former US President Donald Trump last year, has been found effective in a prophylactic study published in a prophylactic study published in the Journal of The Association of Physicians of India (JAPI)
The study showed that hydroxychloroquine, popularly known as HCQ, could prevent SARS-CoV-2 infection in varying degrees depending on its dosing regimen. The highest prevention rate of 72 per cent was found among those given hydroxychloroquine over six weeks or a longer duration.
The study said, “[W]hen adjusted for other risk factors, HCQ dose as per government recommendations, 2-3, 4-5, 6 or more weeks reduced the probability of Covid positivity by 34 per cent, 48 per cent and 72 per cent.”
The study was conducted May-September last year when HCQ was still part of the Union health ministry’s recommendation in treatment protocol for Covid-19, and it began against the backdrop of contesting claims made by authorities and experts including Donald Trump and his advisor Dr Anthony Fauci, the US’s top infectious disease expert.
In March 2020, Donald Trump declared that hydroxichloroquine was a “game changer” drug in the fight against Covid-19. Dr Fauci dismissed the claim citing lack of study and evidence. Despite Fauci’s counter-positioning, Trump continued to be vocal about taking HCQ as prophylactic drug.
Incidentally, the Union health ministry on June 6 dropped hydroxychloroquine from Covid-19 treatment protocol. In its nine-page guidelines released on Sunday (June 6) by the directorate of health services, hydroxychloroquine, ivermectin and favipiravir find no mention.
The government’s decision came on the back of criticism by experts who pointed out a lack of study-based evidence to recommend hydroxychloroquine in Covid-19 cases. The government’s revised guidelines, however, contradicts the recommendations made by the Indian Council of Medical Research as released on May 17.
The ICMR guidelines prescribed the use of hydroxychloroquine in mild cases of Covid-19.
The authors of this prophylactic (relating to prevention of a disease) study said that this “is the largest multicenter study on HCQ prophylaxis on HCWs (healthcare workers), covering over 12,000 HCWs at the risk of Covid-19”.
The study was conducted in May-September last year across 44 hospitals in 17 states involving hundreds of doctors, who received doses of hydroxychloroquine.
One of the co-authors of the study, Dr Raj Kamal Choudhry said, “In the 1985-86 edition of Harrison’s Principles of Internal Medicine [a highly recommended book for students studying medicine in medical colleges], Dr. Fauci wrote that HCQ worked an anti-viral agent despite being an anti-malarial drug. There was no Covid-19 back then, but HCQ’s anti-viral properties were already well known.”
Dr Raj Kamal Choudhry, who was the nodal officer for the prophylaxis study of HCQ in Bihar’s Bhagalpur medical college, said, “We had given about 2,700 doctors and paramedical staff, laundry and kitchen people the prophylaxis of HCQs in the dose of HCQs 400 mg 1×2 for first day then 1 tab daily for 4 days.”
“We did not give to those who had palpitations and had QT prolongation [a measure of heart ailment]. Those who took this drug did not have Covid excepting 5 and 6. The effect was tremendous. Later, we gave this drug to all who had mild cases. Only those patients who were in ICU were not given.”
“Of 2,700 people who were given HCQs, 700 were doctors. Only five or six got infected with SARS-CoV-2 in Bhagalpur but none developed serious complications, and nobody died of Covid-19,” Dr Raj Kamal Choudhry told Indiatoday.in.
The evidence is piling up. There has been numerous, over 50 studies like this showing that HCQ is effective, both as prophylactic, and as an early cure. Yoo bad that the medical bureaucracy considered it more important to get rid of Donald Trump than to save over 100,000 lives in U.S. alone.
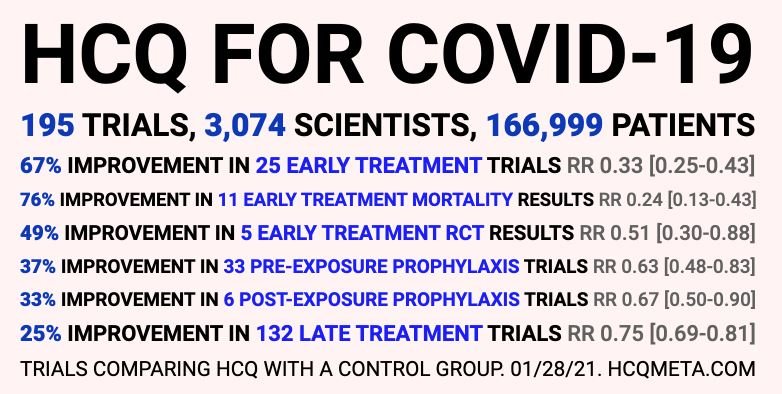
In addition HCQ is too cheap and generic to warrant a double blind study.
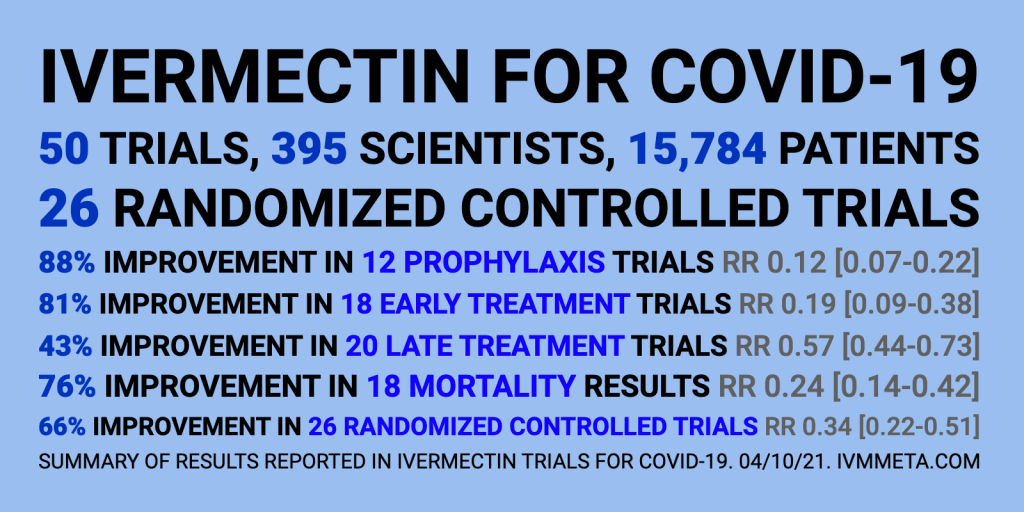
The other medication that may be as effective, and save lives is Ivermectin, an anti-parasite drug used to treat horses and other farm animals. You can buy it at Tractor Supply, so I have been told.
The chairman of the Tokyo Medical Association, Haruo Ozaki, held a press conference August 13, announcing that the anti-parasite medicine Ivermectin seems to be effective at stopping COVID-19 and publicly recommending that all doctors in Japan immediately begin using Ivermectin to treat COVID.
The Journal of Antibiotics a 12 June 2020 report on Ivermectin states: (This is very technical) [https://www.nature.com/articles/s41429-020-0336-z]
“Several studies reported antiviral effects of ivermectin on RNA viruses such as Zika, dengue, yellow fever, West Nile, Hendra, Newcastle, Venezuelan equine encephalitis, chikungunya, Semliki Forest, Sindbis, Avian influenza A, Porcine Reproductive and Respiratory Syndrome, Human immunodeficiency virus type 1, and severe acute respiratory syndrome coronavirus 2.”
Professor Borody says his research has led him to a triple therapy of Ivermectin, zinc and an antibiotic – which are all TGA and FDA approved – which could be the fastest and safest way to stop the Victorian outbreak within 6-8 weeks. [See Professor Borody’s published research papers ORIC here http://orcid.org/0000-0002-0519-4698]
Professor Borody said, “These 3 medications are already approved. They do not need pre-clinical or clinical trials nor additional TGA approvals unless the aim is to combine in a single capsule, for example. Patient treatment programs have been done in the US and elsewhere which indicate it can work within 4-6 days.”
Professor Borody has reviewed the key antiviral scientific research literature and identified the combination of 3 drugs that are in chemists right now and can be prescribed by doctors immediately. The tablets can be taken at home as a preventive treatment by high risk individuals, or by those who test positive to minimise need for hospitalisation at the higher curative dose.
The therapy comprises:
- Ivermectin – TGA and FDA approved as an anti-parasitic therapy with an established safety profile since the 1970s. Known as the “Wonder Drug” from Japan.
- Zinc
- Doxycycline – TGA and FDA approved tetracycline antibiotic that fights infections, such as acne, urinary tract infections, intestinal infections, respiratory infections, eye infections, gonorrhea, chlamydia, syphilis, periodontitis (gum disease), and others.
Professor Borody says distribution teams could be deployed in Victoria’s hotspots to treat proven infected patients immediately, and people exposed or at risk could be taking the preventative dose.
The Governor of Florida, DeSantis is promoting the use of Regeneron. Florida has one of the highest outbreaks of the Delta variant of the Covid-19 virus.
What is Regeneron?
Regeneron, which is being used at all Florida sites, is a common name for REGEN-COV, a monoclonal antibody treatment manufactured by Regeneron Pharmaceuticals.
“It’s the only monoclonal that’s had success against the delta variant,” DeSantis said, adding another benefit is the injections take only minutes instead of an IV that takes an hour. But there is a short window of opportunity.
“You’ve got to do this early, so if you are infected, by the time you get very, very ill and require hospitalization, it’s probably too late for this to work,” he said. “Clearly, the sooner you do it, the better you’re going to be.”

Studies have shown a 70% reduction in hospitalizations among people who have had a monoclonal antibody treatment, DeSantis said.
The treatment isn’t for everyone; REGEN-COV is “an unapproved investigational therapy, and there are limited clinical data available,” the drug’s website cautions.
REGEN-COV is not authorized to treat coronavirus patients who are hospitalized or require oxygen therapy. Citing insufficient data, the manufacturer recommends pregnant women receive the drug only when the benefits outweigh the risks for mother and child.
“Anyone I talked to who had gotten the Regeneron had positive things to say about it,” DeSantis said. “They would just say, ‘I felt so bad, then all of a sudden, I took it and 24 to 48 hours later, I felt much better, my symptoms were resolved.’ You hear that over and over again, and we are hearing it with a lot of the patients that are coming through our sites.”
How are the results so far? See the cases rise and deaths decrease for Florida and judge for yourselves:
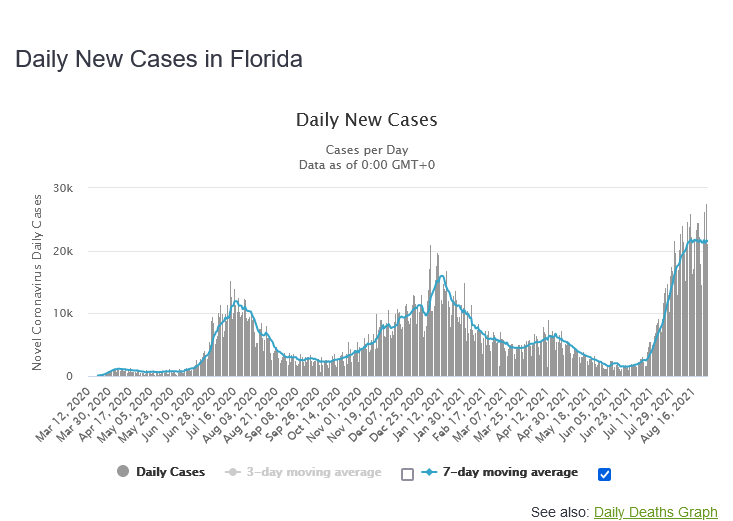
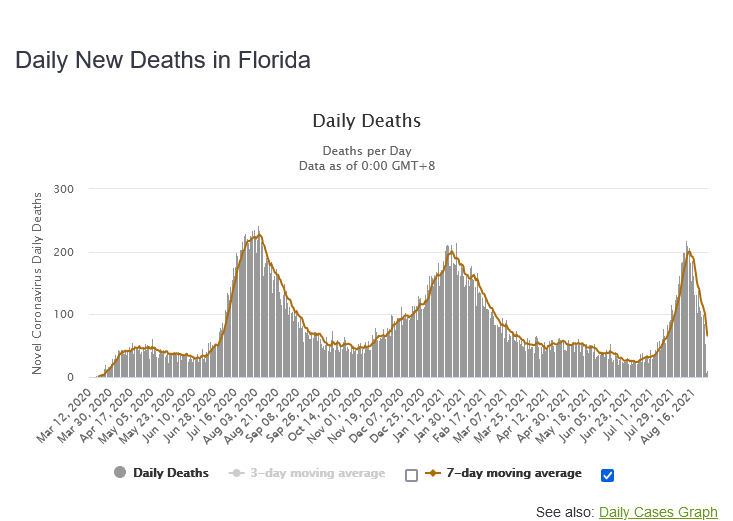
As we can see, deaths plummeted when Regeneron treatment became widely used on seriously ill patients, and the death rate is now 0.32%, going lower.
One more thing, make sure you take supplemental Vitamin D3 (I take 5000 IU/day). An Indonesian study found that the death rate went from 95% if the values were less than 19 nanograms/milliliter to less than 5% if the D3 values were over 31 nanograms/milliliter. The study was made in Covid patients over 65 years old.
Who should get vaccinated? For me, being nearly 80 years old, with a heart condition and a severe blood disease the choice was easy. Of course, I should get vaccinated. But for younger people, people under 45 years of age with a more than 99.9% chance of survival even without HCQ, Ivermectin or Regeneron treatment should they get the Covid.
NEW BLOOMFIELD — A Cleveland Clinic study released this week stated people already infected with the coronavirus gain no additional benefits from vaccination.
The study included 52,000 Cleveland Clinic employees and found not one person who was infected with the virus and chose not to get vaccinated became reinfected.
The data led researchers to conclude those already infected with COVID-19 gain no benefit from getting the vaccine, but an MU Health Care official disagrees with the clinic’s statement.
With this new information my recommendation is to only perform vaccination on demand to preserve personal freedom as much as possible, recommend it to high risk groups, but do not vaccinate children and college age adults! We are close enough to herd immunity to carry out the vaccine trials and prove them effective and safe for the long run before we proceed any further. After all, the vaccines are only approved for emergency use, and children and young adults do not die from it, but the side effects of the vaccine are often much more severe than the disease itself. In children it is mostly asymptomatic. For young adults there is a disturbing rise in the myocarditis after taking the vaccine.

Even if it were correct that HydroxyChloroQuine, Ivermectin and Regeneron monoclonal antibody treatments were highly effective against Covid-19 (it’s not), that still would not mean there is no need to vaccinate people under 45 years of age. That’s because even the most effective therapeutic treatment does not greatly reduce the spread of the disease.
Hundreds of therapeutic protocols are under investigation, and some do seem to be useful, especially the monoclonal antibody cocktails. But no “magic bullet” has been found for treatment of Cov-19, so far.
Vaccination reduces spread of the disease. But since most transmission of Covid-19 occurs before the people who are the sources of the transmissions are even certain that they have the disease, let along begun treatment, so there’s no way for therapeutics to stem the spread of the disease.
HCQ and Ivermectin only work against COVID in conjunction with Zinc. They provide the softening up of the virus membrane, and then the Zinc goes in for the kill. Some people go to Tractor Supply and get a full syringe suitable for a horse inject it and get sick. Don’t do that. Even Dr. Fauci thought that was a bad idea, bad enough to not approve Ivermectin at all. No, the reason I have turned against vaccines for most people under 45 is that the above medications reduce the severity of the disease so much that the death rate from having the disease is lower than from taking the vaccine. If you are over 45 taking the vaccine is better. The study released last week out of Israel showed that the immunity generated by having had the disease is 13 times more effective than taking the vaccine, and the jury is still out how much longer it lasts. With the vaccine they are already talking about booster shots. The second reason is that vaccinated people still get infected with the Delta variety, and when they do they carry many times the virus in their nostrils before symptoms occur, they become super spreaders.
In the first place, it is not correct that the death rate from having the disease is lower than from taking the vaccine.
In the United States the disease has killed 666,627 Americans, that we know of. (That’s from worldometers a few minutes ago.) That’s from 40,871,538 known cases (some of whom remain ill, and will also die), and probably 50-60 million unreported mild cases. That’s a fatality rate of >0.65%.
Additionally, there are hundreds of thousands of Americans who are suffering from lingering (and perhaps permanent) harm, from the disease.
Now, compare that to vaccination. We’ve had 185 million Americans vaccinated for Covid-19, so far, and there are a grand total of three (3) cases, so far, that we know of, in which someone died after getting vaccinated, and in which the circumstances of their death suggest that an unusual response to vaccination was the likely cause. That’s a 0.0000016% fatality rate from vaccination.
Even if there’ve been a few other deaths from vaccination, but not obviously attributable to it, that still means vaccination is around five orders of magnitude less dangerous than getting the disease while unvaccinated.
Note: do not be misled by anti-vaxer liars misrepresenting VAERS statistics. They claim vastly higher death rates from vaccination, but they are lying. This is my comment on that, which I posted on a Whiteboard Doctor video (but which YouTube censored):
In the second place, treatment vs. vaccination is not an “either or” proposition. Being vaccinated doesn’t preclude any treatment options if you have a breakthrough infection — and having been vaccinated greatly improves your chances of avoiding serious illness.
In the third place, even the most effective treatment of the disease could not, even in principle, significantly slow its SPREAD. That’s because most transmission occurs before the source patient is diagnosed, and so before he would be treated. Even if treatment helps him, it cannot act retroactively to prevent him from spreading the disease to others.
Vaccination prevents many infections, and thus reduces the spread of the disease, which therapeutics can never do.
The importance of that is, ironically, proven by the cases in which it fails. Because vaccination is less effective at preventing infections with the Delta variants, those variants are spreading, even as the original variants are fizzling out, and even though vaccination is still preventing most vaccinated people from getting life-threatening cases. Like partially-effective vaccination, or waning but non-zero immunity, effective therapeutics can (theoretically) prevent the disease from become life-threatening. But they can never significantly impede its spread.
That is a very big problem. The spread of Delta variants has caused a huge resurgence of the pandemic, which is killing at least 7000 people per day, in large part because only about 1/3 of the people in the world are vaccinated against Covid-19.
In the fourth place, it is not true that when vaccinated people have “breakthrough” Delta variant infections they “carry many times the virus in their nostrils” or are more likely to “become super spreaders.”
I don’t know which anti-vaxer made up that lie, but it is not even plausible. How could that even work?
The viral loads in vaccinated breakthrough infections vs. unvaccinated have been studied. Here’s a preprint:
Here’s an article about it:
https://www.cbsnews.com/news/covid-vaccine-delta-variant-infections-carry-same-virus-load-unvaccinated/
The bottom line is that if you have immunity (either through vaccination or by surviving the disease) you are much less likely to spread the disease to other people than if you are unvaccinated. The anti-vaxers who claim the opposite are just plain lying.
In the fifth place, you’ve been misled about the effectiveness of HCQ and ivermectin. Neither of them are “silver bullets.”
Ivermectin is more promising than HCQ; here’s a review:
https://pubmed.ncbi.nlm.nih.gov/34318930/
It says, “evidence on efficacy and safety of ivermectin for prevention of SARS-CoV-2 infection and COVID-19 treatment is conflicting.”
(OTOH, there’s nothing “conflicting” about the conclusive evidence that vaccination against Covid-19 is extremely beneficial!)
There’s a LOT of misinformation being circulated about ivermectin, and that “ivmmeta” site you cited is a major source of it. “Health Nerd” sent out an informative 39-part tweetstorm about it. Here’s the first tweet:
Here’s a compilation:
https://rattibha.com/thread/1422044335076306947?lang=en
There is some evidence (far from conclusive) that ivermectin might have some benefit for Covid-19 patients, but anyone who tells you that you should take ivermectin instead of getting vaccinated is trying to kill you.
What’s more, even if ivermectin (and/or some other therapy) were found to be very helpful for Covid-19 patients, vaccination would still be necessary, simply because immunity to the disease, by vaccination or by surviving an infection, limits its spread, and merely treating the disease cannot.
So if you don’t yet have Covid-19 antibodies (either through vaccination or “the hard way,” by surviving the disease), please get vaccinated ASAP.
Oops, I accidentally left out the link to the preprint:
Click to access finalfinalcombinedve20210816.pdf
Sorry about that!
Thank you again Dave for valuable commenting.
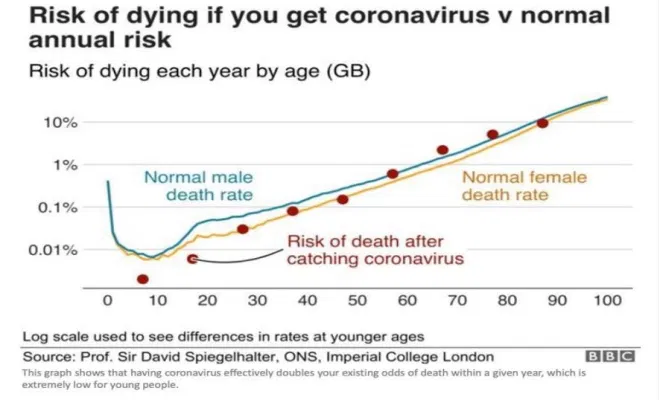
For me the situation was easy. Being 80 years old with a stent and a fairly complicated anemia I had a 7% risk of dying if I should get COVID. My wife had a 5% risk. So we put ourselves in the waiting line for vaccine and finally got it. The risk of dying from COVID decreases by about 7% per year in a near perfect exponential decline, so that in he U.S.A. the COVID-19 deaths 2020-21 by age (year) was:
– 30% of all deaths occurred over the age of 85
– 80% of all deaths occurred over the age of 65
– Only 15% of the U.S. population is over the age of 65
0.02% of all deaths occurred under the age of 2, too young to get vaccine
0.05% of all deaths occurred between the ages of 2 and 18, school age
0.15% of all deaths occurred between the ages of 19 and 25, college age
3.6% of all deaths occurred between the ages of 26 and 45
(Source: CDC – just updated: https://data.cdc.gov/NCHS/AH-Provisional-COVID-19-Death-Counts-by-Age-in-Yea/3apk-4u4f )
Armed with these facts, and remembering well the Thalidomide catastrophe in Europe, because they approved the drug before a full pregnancy cycle had occurred. The result was miscarriages, braindead babies, missing limbs or fingers dependent on which day of the pregnancy you took the drug. So I would hold off on the final approval of the vaccine until a full cycle is completed. For children 2 to 18 years more die from flu in a normal flu year than died from COVID. The results from Israel is that the majority of new hospitalizations from covid was that over 70 percent came from fully vaccinated patients, but that is somewhat misleading since the vaccinated population is older, so fully vaccinated people are four times better off than the unvaccinated. And the average severity is less. With all this said, this is my recommendation: All people over 45 should be highly encouraged to take the vaccine. Between 25 and 45 only people in the high risk category should get it, for everybody else it is optional. Under age 25 only very high risk people should get the vaccine. If anyone has natural immunity , they should not get vaccinated again. This is where I stand today. When the results are finally in I may change my mind according to science.