Let us take a look at the nations that have country wide use of Ivermectin and see how they fare compared to the nations that don’t.
Bangladesh have been using Ivermectin since June 2020. Population 167 million. Total deaths per million 168. COVID-19 cases are down 99% from peak, deaths down 98%
Belize has been using Ivermectin since 2020, but only for serious cases. Population 0.4 million. Total deaths per million 1,450. COVID-19 cases are down 89% from peak, deaths down 67%
Bolivia has country-wide usage. Population 12 million. Total deaths per million 1,641. COVID-19 cases are down 70% from peak, deaths down 59%. Less than half of the population are vaccinated.
Bulgaria has country-wide usage. Population 6.8 million. Total deaths per million 4,450. COVID-19 cases are down 36% from peak, deaths down 80%. Bulgaria had a late start with vaccines and has still the lowest vaccination rate in Europe of 32.4%.
Cambodia has country-wide usage. Population 17 million. Total deaths per million 176. COVID-19 cases are down 99.5% from peak, deaths down 75%
Dominican Republic – country-wide adoption – Sep 30, 2020. Population 11 million. Total deaths per million 385. COVID-19 cases are down 76% from peak, deaths down 90%
Egypt – country-wide adoption – Nov 30, 2020. Population 105 million. Total deaths per million 205. COVID-19 cases are down 38% from peak, deaths down 44%
El Salvador – country-wide adoption. Population 12 million. Total deaths per million 1,641. COVID-19 cases are down 36% from peak, deaths down 80%
Guatemala – country-wide adoption – Jan 23, 2021. Population 12 million. Total deaths per million 1,641. COVID-19 cases are down 95% from peak, deaths down 80%
Honduras – country-wide adoption – Apr 23, 2020. Population 8.5 million. Total deaths per million 875. COVID-19 cases are down 36% from peak, deaths down 92%
Lebanon – country-wide adoption – Jan 27, 2021. Population 6.8 million. Total deaths per million 1,334. COVID-19 cases are down 48% from peak, deaths down 62%
Nicaragua – country-wide adoption – Jan 25, 2021.Population 6.7 million. Total deaths per million 31. COVID-19 cases are down 92% from peak, deaths down 50%. This number is highly suspicious.
Panama – country-wide adoption. Population 4.4 million. Total deaths per million 1,680. COVID-19 cases are down 40% from peak, deaths down 80%
Venezuela – country-wide adoption.Population 28 million. Total deaths per million 188. COVID-19 cases are down 83% from peak, deaths down 80%
But the most interesting aspect of the first picture is what happens to the countries that use Ivermectin to fight parasites such as river blindness or head lice just to name a few. Look at this chart!
This chart lists Egypt as non Ivermectin because it is not used to fight parasites, but the point is clear. Ivermectin is working well as a prophylactic for COVID-19 even though its intent is to fight parasites. The death rates being around 90% lower for countries that fight parasites should be enough evidence for any thinking individual.
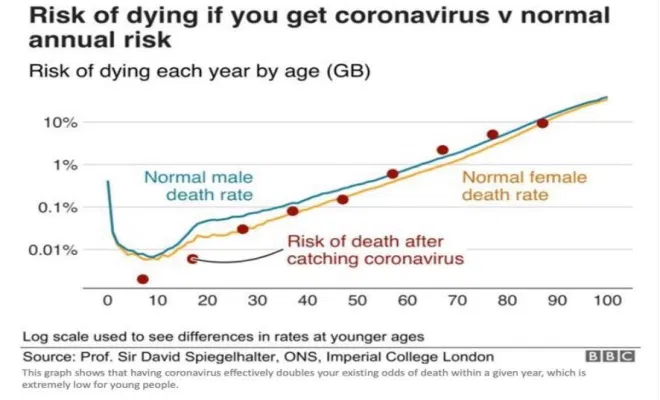
So here is my suggestion: Vaccines help for older people and people with special risk factors. The death rate for COVID-19 rises by about 7% par year of age after 2 years. See chart:
The statistics from the U.K. Office for National Statistics shows a 2.2x higher death rate for fully vaccinated people under 60 years of age than for unvaccinated people.
Charting these statistice I find that the crossover age is 45 years. People under this age are better off taking Ivermectin than get vaccinated unless there are special risk factors. Since between 2 and 3 billion people are already taking it for parasite protection it cannot be that dangerous. And by the way Ivermectin was offered to all Afghan refugees, as per immigration protocol, not for COVID, but for parasite control.
Summary: For people over 45 years of age and anybody with special risk factors. Take the vaccine, and continue with boosters. At the earliest sign of COVID take Ivermectin, Zinc and an antibiotic.
For the rest, most people under the age of 45, take Ivermectin and Zinc and an antibiotic during the first 5 days of symptoms, If diagnosed later there is most hopefully Regeneron available.
This would reduce the death rate by 80 t0 85%, reduce hospitalizations by a lot and make COVID-19 a mere nuisance so we can return to a normal life.
The EU’s drug watchdog on November 19 backed Merck’s anti-COVID pill for emergency use ahead of its formal authorization and started reviewing Pfizer’s antiviral treatment as cases soar across Europe.
The two pills by the US pharma giants represent a potentially groundbreaking step in the fight against coronavirus as studies show they cut the risk of hospitalization and death in high-risk patients.
The European Medicines Agency (EMA) said that while the Merck pill was not yet approved, it had “issued advice” so that individual countries in the 27-nation EU could decide whether to use it in case of a surge in infections.
The EU’s drug regulator on Dec 16 allowed member states to use Pfizer’s new COVID pill ahead of its formal approval, as an emergency measure to curb an Omicron-fuelled wave.
Pills like those by US pharma giant Pfizer and rival Merck have been hailed as groundbreaking because they do not need to be injected or taken intravenously, making them more accessible.
Pfizer said this week that its Paxlovid pill reduced hospitalisations and deaths in vulnerable people by almost 90 percent.
“The medicine, which is not yet authorised in the EU, can be used to treat adults with COVID-19 who do not require supplemental oxygen and who are at increased risk of progressing to severe disease,” the EMA said in a statement.
“EMA issued this advice to support national authorities who may decide on possible early use of the medicine… for example in emergency use settings, in the light of rising rates of infection and deaths due to COVID-19 across the EU.”
Merck’s pill decreases the ability of the coronavirus to multiply by increasing the number of mutations in its genetic material (or RNA).
The Pfizer pill uses a different method, belonging to a class of antivirals called “protease inhibitors”, which block the action of an enzyme that is critical to viral replication.
It is a combination of a new molecule, PF-07321332, and HIV antiviral ritonavir.
Europe has been searching for whatever methods it can to curb a fourth wave of COVID cases that has already prompted several countries to tighten restrictions.
Why not approve Ivermectin?
When a new epidemic breaks out, one for which there is no approved medication available that will cure the patient it has always been the aim of the medical community to see if there are any approved drugs that can be repurposed to cure the patient, because it takes too long to develop brand new drugs.
When the COVID-19 pandemic broke out there was a wild scramble to see what other drugs were available, most of it in other countries. One such effort, in Marseille, France, by a Muslim doctor caught the attention of then President Trump, and he started promoting it. It involved Hydrochloroquine, Zinc and Azithromycine, and it worked remarkably well when taken early, people were cured in 5 days, but it had one fatal flaw, the main drug is generic, and therefore the medical-industrial complex could not make any money on it, so no studies in the U.S.A could be performed by it and so, it could not be approved. Plus, it had been promoted by Trump, and he was no medical expert. Many countries with limited medical budgets called on its wide use as an early treatment with good results, the death rate of these, mostly developing countries was substantially lower than the advanced countries. Here is some early evidence.
The sub-Saharan countries that are plagued by river blindness had almost no COVID cases early during the pandemic, but no- one noticed. It turns out that in those countries they are using Ivermectin to prevent river blindness. This also blocks COVID-19, and so, Ivermectin was inadvertently repurposed. How successful is it? The data is here. India and Indonesia have drastically reduced their COVID-19 cases by the use of Ivermectin, results here. Japan reducrd their COVID-cases by 99%, see here.
. it works the same way as IverThe results speaks for themselves, that is for everybody except NIH, CDC and FDA. To protect their investment in COVID-19 disease management Pfizer is coming out with a pill, PF-07321332 which has been dubbed Pfizermectin by the social media, and for good reason, it works the same way as Ivermectin, but the molecule used is quite different. It is more specifically targeted at COVID-19, delta variant, and as such is even more efficient than Ivermectin, but Ivermectin is more broadband, and may work well against all future mutations of the virus and even against the next pandemic in the COVID family. The great advantage of the Pfizer pill is that it is expensive and as such will be approved lickety-split,, whereas the true cost in Africa for the Ivermectin pill is 6 cents.
Anyhow, here is Dr, John Campbell with the best presentation of how Ivermectin works I have seen. It has many scientific references.
A large medical study of seniors, both Viagra users and non users (7.2 million seniors medical records were scanned for six years by the Cleveland Clinic) and they found that Viagra users were 69% less likely to develop Alzheimer disease. This was interesting. Did they find anything else? Less Cancer, less Parkinson’s disease?
Could there be something else that made a difference? Viagra itself was developed to be a blood pressure lowering drug by expanding the blood vessels. During the early trials they found that it had some unexpected side effects. For some, the side effects were desirable, so they repurposed the drug, and Pfizer racked up about 15 Billion dollars in sales until the patent expired in 2020. It is now generic under the name sildenafil. There is only one problem with this. To repurpose a drug, in this case against Alzheimer you have to have a control group that is not aware that they are given a placebo, which is not possible in this case. Plus it is now generic, so there is no interest in doing a double blind study for economic reasons, it no longer fits the medical industry’s business model.
Many years ago I saw a nicely framed plug for flossing in my dentist’s office. It said: People who floss every day live on average seven years longer. This may very well be true, but could it also be because people who floss take care of themselves in many other ways?
A long time ago there was a study that established a strong correlation between circumcision and prostate cancer. People who were not circumcised had a much higher incident of prostate cancer, case closed, get circumcised. There was only one problem with the study: It was taken mostly in Minnesota with a large Scandinavian population. Scandinavians do not get circumcised as a rule, and they are genetically much more prone to get prostate cancer than other people. When the genetic variations are taken out, there is no difference between circumcision, non circumcision and cancer.
Which brings me to COVID-19 and why more pigmented people are more likely to suffer, even die from COVID-19. The first excuse is that they get an inferior health care because we are a deeply racist society. There are a couple of other possibilities. An Indonesian study showed a strong correlation between Vitamin D levels and fatal outcome for older people with COVID-19. If the level was below 27 ng/ml the death rate was over 80%, if the level was over 31 ng/ml the death rate was less than 10%. See: https://lenbilen.com/2020/12/27/vitamin-d-as-covid-19-fighter-a-most-important-virus-fighter/
Another possibility is there are genetic differences between people of dark complexion and pale-skinned people. It is through genetic differences we determine our ancestry, it has become widely popular, so it is not in and of itself racist to look into one’s roots. It turns out that the rate of COVID-19 in equatorial Africa is much lower than in U.S. In Africa there was a debilitating illness called river blindness. The parasite killer Ivermectin, originally developed against parasites in horses and as heart worm killer in dogs proved effective against river blindness, and so it became widely distibuted in Central Africa. The countries that use Ivermectin have around one tenth of the cases than the countries of North and Southern Africa. It seems that Ivermectin had been inadvertently repurposed to fight COVID-19. See: https://lenbilen.com/2020/12/27/vitamin-d-as-covid-19-fighter-a-most-important-virus-fighter/
To test this hypothesis Indonesia, India and Japan did introduced Ivermectin as the primary early prophylactic and therapeutic COVID-19 fighter. The results are startling, Indonesia has seen new cases drop 99.5% and deahs drop 99.4% since the peak before introduction of Ivermectin. The corresponding numbers for India are 98% and 93.3%, but in Uttar Pradesh and Delhi the results are much better. In Japan the cases are down 99.5% and deaths are down 98.4%.
Can the U.S. achieve similar successes by repurpose Ivermectin to fight COVID-19? It is a strong virus killer, and it is more broadband than the mRNA vaccines. The vaccines work too as a Prophylactic Therapeutic for a season, but is what they call leaky insofar that they are more specific and make possible an occasional vaccine resistant mutation to develop, and so a vaccine booster variant has to be developed and distributed, thus satisfying the medical industry’s business model, first do not cure the patient, but maintain stable control and assure the patient of a long life of dependency.
The other buisness model advocared by the medical doctors and nurses is that they really want to cure the patient. Ivermectin will go a long way to achieve that goal. Just think, reducing COVID hospitalizations and deaths by a modest 90% in about seven weeks after Ivermectin is fully approved would change things.
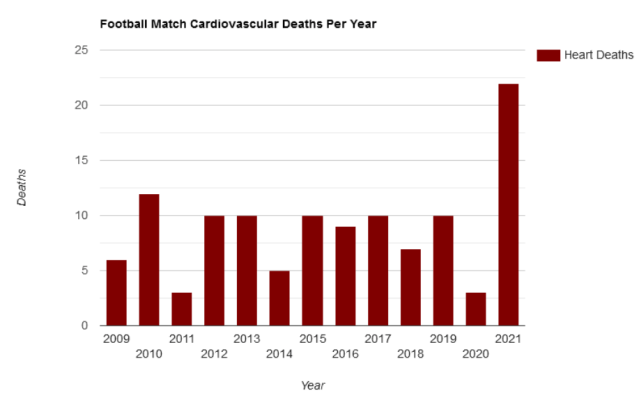
An investigation of available data shows that worldwide football / soccer match cardiovascular deaths in 2021 are 278% higher than the 12-year average, and analysis further indicates that the vast majority of excess mortality in the UK this year has been due to cardiovascular, immunological and neurological damage caused by the Covid-19 injections.
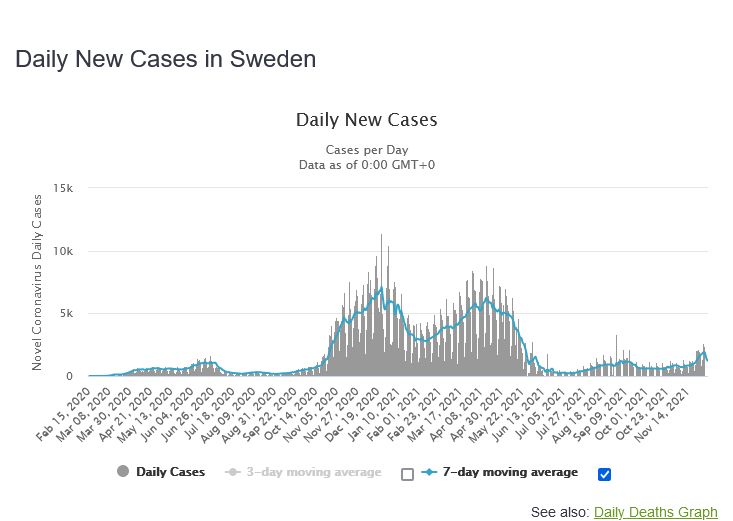
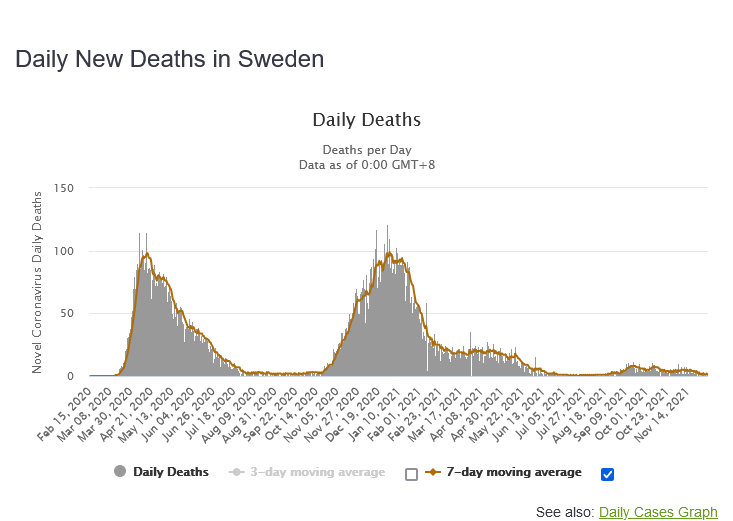
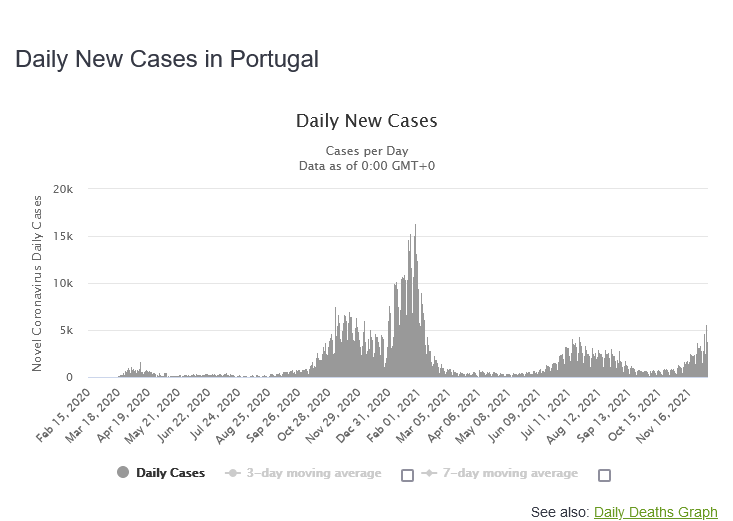
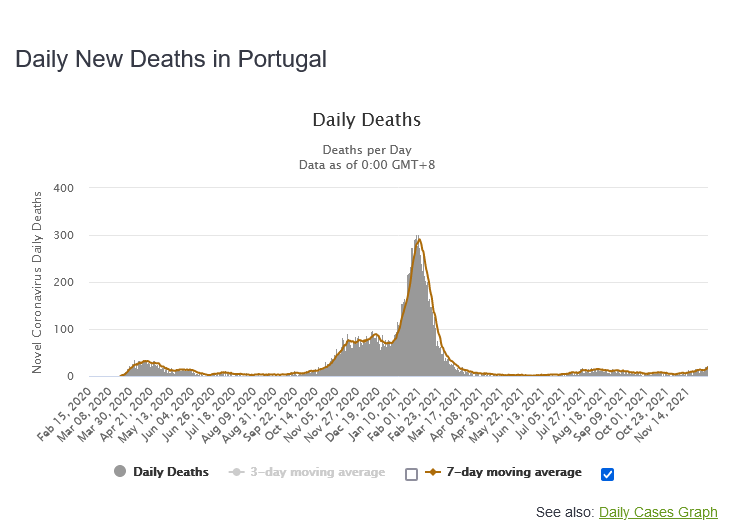
When the COVID-19 menace entered Europe, Sweden was the only country that didn’t do a complete lock-down, they took the approach to let the pandemic rage and so achieve herd immunity; only protect the most vulnerable as best they could. The initial result seemed catastrophic, but herd immunity was more or less achieved, and current results are impressive:
As we can see, for Sweden daily deaths are down 98% from.previous maximum before vaccines began, and daily cases were down 83%. The total death rate per million people is 1,480 and the Swedish vaccination rate is 72%
How are the other European nations doing on the same score. They are listed in order of Increase/decrease in death rate from pre-vaccine peak, from worst to best.
A= ratio of highest case rate before vaccines to current case rate
B= ratio of highest death rate before vaccines to current death rate
C= total deaths per million people this far
D= vaccination rate, at least one dose
Country A B C D
Ukraine 155% 299% 2,036 29%
Russia 114% 218% 1,926 43%
Belarus 90% 167% 548 33%
Georgia 93% 142% 3,119 28%
Finland 314% 140% 249 77%
Hungary 176% 102% 3,649 62%
Greece 223% 90% 1,797 66%
Croatia 112% 82% 2,769 51%
Moldova 37% 81% 2,292 14%
Serbia 26% 81% 1,372 47%
Slovakia 346% 78% 2,727 47%
Latvia 80% 76% 2,304 67%
Bulgaria 58% 76% 4,197 16%
Poland 90% 76% 2,267 54%
Bosnia & H. 53% 71% 3,930 26%
Montenegro 38% 63% 3,708 42%
Chechia 150% 52% 3.135 60%
Norway 528% 50% 199 77%
Romania 16% 50% 2,997 29%
Netherlands 193% 49% 1,144 77%
Lithuania 56% 47% 2,572 69%
Austria 121% 46% 1,409 68%
N. Macedonia 31% 45% 3,668 42%
Estonia 80% 43% 1,374 62%
Slovenia 89% 30% 2,557 58%
Germany 229% 34% 1,231 70%
Denmark 122% 34% 508 78%
Slovenia 89% 30% 2,557 58%
Albania 40% 25% 1,082 32%
Belgium 104% 24% 2,330 75%
Switzerland 98% 15% 1,328 67%
France 80% 14% 1,826 76%
Ireland 80% 13% 1,138 77%
Italy 41% 10% 2,224 78%
U.K. 77% 9% 2,129 74%
Spain 34% 6% 1,885 82% .
Portugal 21% 6% 1,800 89%
Conclusion: All countries will eventually reach herd immunity, the vaccinations only delay the inevitable: The pandemic will be with us like the common cold or the flu.
This document provides an integrated analysis of the cumulative post-authorization safety data, including U.S. and foreign post-authorization adverse event reports received through 28 February 2021.
The document reveals that within just 90 days after the EUA release of Pfizer’s mRNA vaccine, the company was already aware of voluntary adverse reaction reports that revealed 1,223 deaths and over 42,000 adverse reports describing a total of 158,893 adverse reactions. The reports originated from numerous countries, including the United States, United Kingdom, Italy, Germany, France, Portugal, Spain and other nations.
Of special interest is what happens to pregnant and breastfeeding mothers
This is alarming, since a gestation period is 9 months, and these are snapshots the first 90 days after introducing the vaccine. The question that many women have, especially health care women that have seen what is going on is: How safe is this vaccine really? Will it cause infertility? Will it drastically increase stillbirth? Will it damage my child in the womb? We now have nearly a year of data, and no one comes out and assures us that none of these things are happening, just an increase in deaths, and a large number of adverse reactions.
The second set of questions are: How much worse is COVID-19 itself compared to the vaccine? Does COVID-19 cause infertility? Is blood clotting worse? It maybe that for children and young adults the vaccine is worse than COVID itself, other data seems to suggest so for people under 45 years of age.
This vaccine should be halted for people under age 45 until answers are given. There seems to be a benefit for older people, a substantially reduced death risk.
BNT162b2 5.3.6 Cumulative Analysis of Post-authorization Adverse Event Reports CONFIDENTIAL Page 1 APPENDIX 1. LIST OF ADVERSE EVENTS OF SPECIAL INTEREST 1p36 deletion syndrome; 2-Hydroxyglutaric aciduria; 5’nucleotidase increased;
November 3, 2021, San Diego, County Board of Supervisors meeting. Dr Scot Youngblood MD.
7:32 video of a doctor decimating the vaccine narrative at the San Diego county board of supervisors meeting. Worth the watch and forward to all.
This talk was given before the arrival of the Covid-19 Omicron variant. An ominous warning is coming from the Isle of Man Chief Minister Alf Cannan: “The greatest concern is that the virus has mutated to such an extent that our immune systems, trained by the vaccine, no longer recognize the virus and no longer trigger an immune response. This sort of variant is called an immune escape variant. Early evidence suggests there may be a higher infection risk with Omicron.”
If that is true, who should then get the vaccine, and should we push the booster shot?
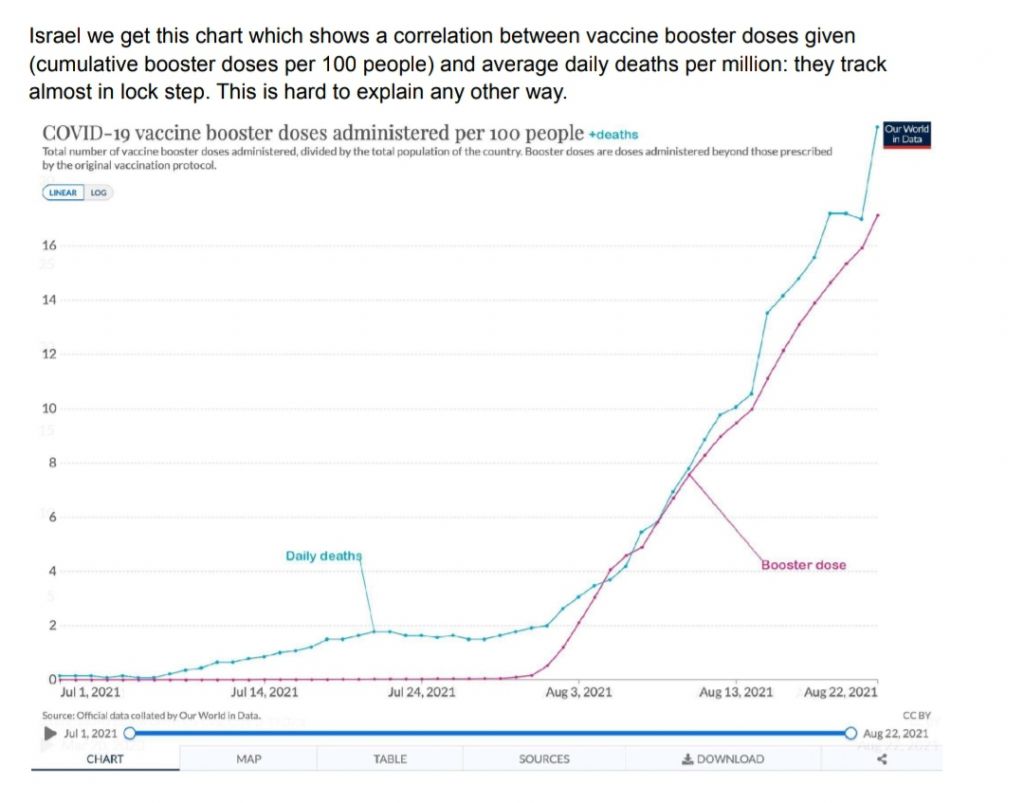
Here is another ominous chart from Israel, having a very high vaccination rate among Jews, mostly with the Pfizer vaccine. The younger Arab population has only half the vaccination rate, and logically they have twice the COVID case rate. Israel was the earliest to vaccinate, and in August was ready to do booster shots. The results: More vaccination deaths.
The results were so alarming that they nearly stopped the booster shots, awaiting further evaluation
Looking at death risk versus age, it seems logical that older people benefit from the vaccine. This chart is from 2020, without any vaccines available.
But no we know so much more. The VAERS data, while abundant is not readily available, but U.K. and Scotland publicize the results, and it is abundantly clear that what we have here is vaccines that are failing. While they reduce the symptoms for a fully vaccinated person the vaccine do not immunize but instead acts as a potential mutation agent for the infected person, and thus once in a while a new variant is born.
The problem is that the vaccines are too specific, and allow mutations to escape, much like specific antibiotics, while very effective in the beginning, once in a while a resistant mutation develops, rendering the antibiotic useless. We need to go back to the drawing board and develop more broadband vaccines. The mRNA method of combating diseases has a bright future, not as a vaccine, but to fight cancer. The field is wide open, and the technology is well advanced.
Meanwhile we should go back and fight COVID-19 the old fashioned way, with proven medications suggested here. In the meantime, if you are fully vaccinated and over 45, it is o.k. to take the booster vaccine. It will increase the individual protection, but the transmission risk remains.
There is a new COVID variant, the Omicron. The stock markets around the world show they are worried, Crude oil futures dipped 13% in one day, fear spread through the media, and the message is as always: Get vaccinated, get the booster shot if you are eligible, but above all, trust us!
The news from Botswana is interesting to say the least. When testing passengers prior to departure they found that four future passengers tested positive for the Omicron variant.
Botswana is a large country but with only 2.4 million people. It is the fourth wealthiest country in Africa, and its health system is good, but only 20% of the population is fully vaccinated. Here is the kicker: All 4 of the infected were fully vaccinated!
This means that vaccinated people are potential “Typhoid Marys”, and while the vaccine protects them from the worst effects of Covid-19, they are just as dangerous as unvaccinated covid-19 patients, probably more so, since they can share a much higher viral dose before symptoms show .
In the summer of 2021 Botswana toyed with using Ivermectin, but decided against openly advocating it. They accepted its use as a prophylactic and early intervention drug, and the daily new cases and deaths dropped 97%. Then on Thanksgiving these bad news arrived.
President Biden reacted with historical speed. Starting Monday he will ban all travel from South Africa and Botswana, all predominantly racially black countries. He didn’t want to ruin the long Thanksgiving holiday, he must allow some time to let the virus enter U.S. before instituting the travel ban.
There are better alternatives. India, Indonesia and Japan are using Ivermectin to eradicate the virus, at great success. Can we do the same thing?
Yes we can! NIH has approved Ivermectin for controlled use, see document here.
CDC is really a vaccine producing agency, they control more than 20 patents, so they cannot profitably participate, even doing so would have saved and will save hundred of thousands of lives.
Bad news about the dangers that mRNA vaccines may pose to the heart and blood vessels keeps coming.
A new study of 566 patients who received either the Pfizer or Moderna vaccines shows that signs of cardiovascular damage soared following the shots. The risk of heart attacks or other severe coronary problems more than doubled months after the vaccines were administered, based on changes in markers of inflammation and other cell damage.
Patients had a 1 in 4 risk for severe problems after the vaccines, compared to 1 in 9 before.
Dr. Steven Gundry, a Nebraska physician and retired cardiac surgeon, presented the findings at the Scientific Sessions of the American Heart Association’s annual conference in Boston last week. An abstract is available in Circulation, the AHA’s scientific journal.
My conclusion from that statistics is that vaccines are beneficial if you are over the age of 46. Because of the coarseness in the age-related data, only 4 categories, the uncertainity is +- 5 years. This is one more argument that speaks for the conclusion that if you are young, you are better off getting COVID-19 and acquiring natural immunity, rather than take the vaccine and be stuck with booster shots every 6 to 8 months. The vaccine itself is experimental, and we do not yet know the long term effect of it, much less the long term effect of the booster shots.
Vaccinated English adults under 60 are dying at twice the rate of unvaccinated people the same age
And have been for six months. This chart may seem unbelievable or impossible, but it’s correct, based on weekly data from the British government. The brown line represents weekly deaths from all causes of vaccinated people aged 10-59, per 100,000 people. The blue line represents weekly deaths from all causes of unvaccinated people per 100,000 in the same age range. This graph is correct. Vaccinated people under 60 are twice as likely to die as unvaccinated people. And overall deaths in Britain are running well above normal. The basic data is available here, download the Excel file and see table 4:
This new data set indicates a sharp rise in overall mortality from all cases as people get older it was given as 2 categories, unvaccinated and those having received 2 doses of vaccine, broken up in 10-60, 61-70, 71-80, and 80+ years age groups, coarse but usable categorization. This indicates a decrease in deaths of 45% for people 61-70, 46% for the age group 71-80, and 33% for people 80 and over. All these numbers jump widely so the confidence interval is only about 10%. Massaging the data as best I could with this limited set I came up with the age of 46 years as the crossover point, above which vaccines are preferable.
The conclusion is this: People over the age of 46 should be encouraged to get vaccinated, people under the age of 46 should only get vaccinated if they are in the vulnerable category, and only with a physician’s recommendation.