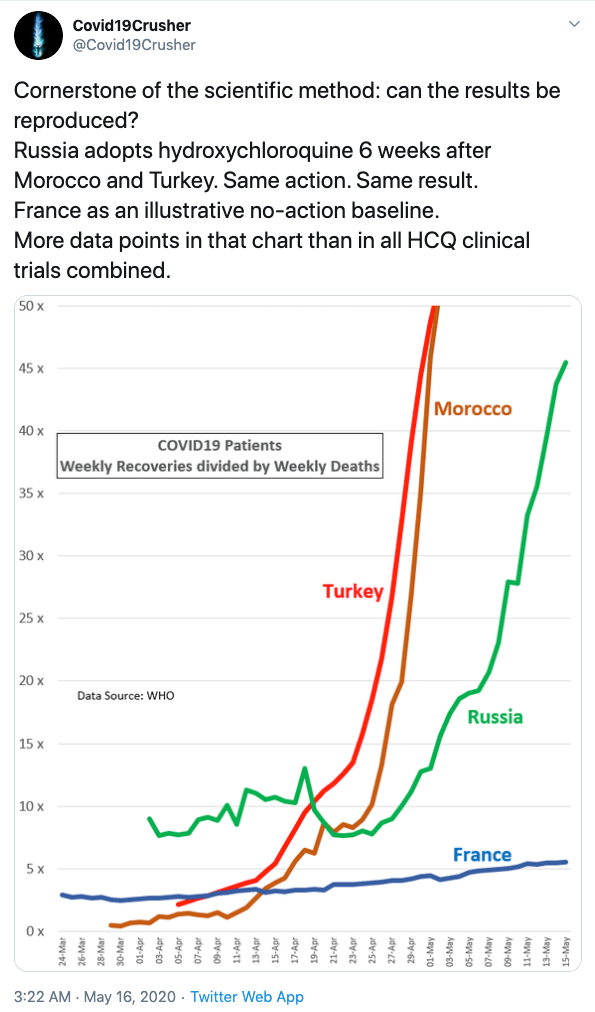
There are at least ten countries that prescribe HydroxyCloroQuine, mostly in combination with Zinc and an antibiotic, as soon as COVID symptoms occur. When the illness has progressed to the point of autoimmune overreaction and the oxygen exchange is to the point of collapse it is too late and may even aggravate the situation.
How are these countries faring in the Corona-virus fight, compared to the rest of the world?
For the world as a whole, the death rate from the Corona-virus as of June 25 is 5.06% of diagnosed cases. and recovered cases versus deaths is 10.74 recorded recoveries for every death.
For the United States the death rate from the Corona-virus as of June 25 is 5.00% of diagnosed cases. and recovered cases versus deaths is 8.37 recorded recoveries for every death. or about the same as for the world as a whole.
Taking the average, adjusted for the number of positive cases, the average adjusted death rate for countries, where people are taking HCQ + Zinc as soon as they are diagnosed positive, is 1.49%.
This means that the risk of death is reduced by a factor of 3.4 if HZQ + Zinc is taken as early as possible after a positive diagnosis for corona-virus!
Recovered cases versus deaths is an indicator of how fast patients recover after taking HCQ. Taking the average recovery ratio over the number of cases, gives the median recovery ratio, of 54.3, compared to the recovery rate for the rest of the world of 10.74, an improvement of 5.1 times as many recorded recoveries for every death. This is an indicator of how fast people recover, but is a very lagging indicator, since many countries do not report recovered cases in a timely manner. If they did, both the numbers for the ten countries, and for the world as a whole would look better, but it is the best measurement we have for now.
The total positive cases for these ten countries are over one million, or about 10.3% of all positive tests so far, far more than any double blind controlled study could ever produce, and indicates that if implemented all across U.S. (and the world as a whole) the death rate from now on would be less than a third of what we are now experiencing. In addition hospitalizations would be greatly reduced.
WHO paused a double blind study out of an “abundance of caution”.
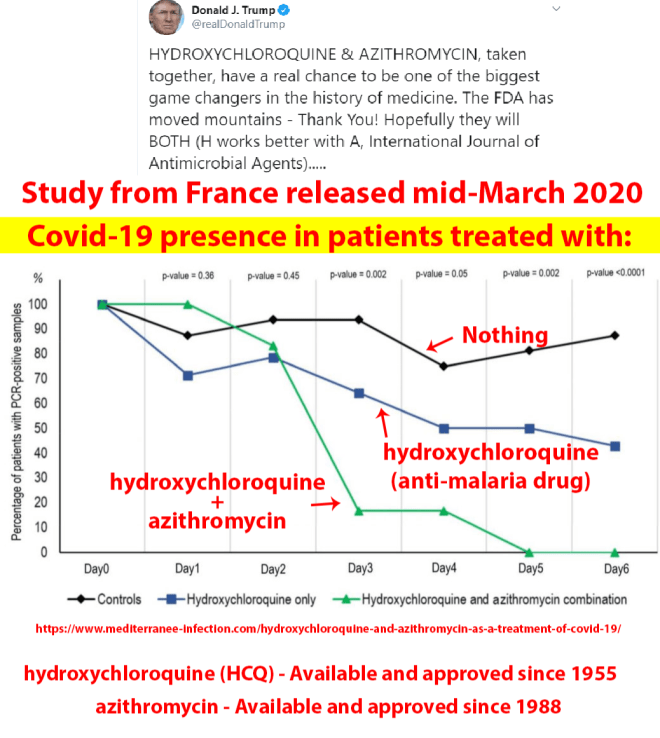
HCQ has been taken by over one million patients testing positive for the corona-virus as soon as symptoms did arise or shortly thereafter. We do not need a double blind control study, the results speak for themselves.
Is it because it has been promoted by President Trump, and some would rather die than get cured because of that?
Is HCQ too cheap to promote? It is totally generic, no pharmaceutical company stands to gain from producing it, so there will be no study made by them. Any study will have to come from government.
Is it too dangerous? No, it is approved and has been given as a prevention for malaria for over 50 years, it has been approved for combating Lupus for over 20 years, and can be given to pregnant women and nursing mothers with no restrictions. There is a small number of cases involving heart arrhythmia, but these patients can be monitored with an ECG, and if the condition is severe they can be advised not to take the medication.
I for one want to save lives.
Appendix: The data is used from https://www.worldometers.info/coronavirus/
The death rate from all causes doubles for every 8 years as you age or about 9% per year. The death rate from Corona-virus is remarkably the same as the death rate from all causes, adjusted for age. The world median age is 30.4 years. So let the world death rate be the norm and adjust for the median age for the 10 countries.
World death rate as of June 25 is 5.06% of diagnosed cases. and recovered cases versus deaths is 10.74
Compare this with 10 countries that use HCQ for most patients as soon as they test positive for the corona virus.
Turkey: Death rate 2.60%, median age 30.9, adjusted death rate 2.48%, recovered cases versus deaths 30.8, total cases 193.115
South Korea: Death rate 2.24%, median age 30.9, adjusted death rate 2.15% recovered cases versus deaths 38.9, total cases 12,563
Malaysia: Death rate 1.41%, median age 28.5, adjusted death rate 1.69% recovered cases versus deaths 68.3, total cases 8,600
Senegal: Death rate 1.50%, median age 18.8, adjusted death rate 4.04%, recovered cases versus deaths 44.2, total cases 6,233
Costa Rica: Death rate 0.45%, median age 31.3, adjusted death rate 0.43%, recovered cases versus deaths 102.2, total cases 2,684
United Arab emirates: Death rate 0.66%, median age 30.9, adjusted death rate 0.63%, recovered cases versus deaths 114.1 , total cases 46,563
Bahrain: Death rate 0.29%, median age 32.3, adjusted death rate 0.25%, recovered cases versus deaths 260.6, total cases 24081
Morocco: Death rate 1.91%, median age 29.3, adjusted death rate 2.08%, recovered cases versus deaths 39.1, total cases 11,338
Russia: Death rate 1.40%, median age 30.9, adjusted death rate 1.34%, recovered cases versus deaths 43.6, total cases 613,994
Qatar: Death rate 0.11%, median age 30.9, but since 88% of the population are migrant workers between 20 and 60, the adjusted death rate is at least 8 times higher, or 0.88 %, and adjusted recovered cases versus deaths 87.9, total cases 91,838