The trend of the five worst and the five best states of Covid-19 death rates versus percent of population tested:
State death rate trend percentage of population tested
. May 8 May 11 up/down May 8 May 11
- Michigan 9.48% 9.64% up 2.4% 3.1%
2. Connecticut 8,87% 8.91% up 3.1% 3.7%
3. New York 7.80% 7.80% __ 5.6% 6.2%
4. Lousiana 7.23% 7.32% up 4.4% 4.9%
5. New Jersey 6.55% 6.71% up 4.4% 4.9%
….
46. Tennessee 1.66% 1.61% down 3.4% 4.0%
47. Nebraska 1.17% 1.16% down 2.0% 2.5%
48. Wyoming 1.08% 1.05% down 2.1% 2.3%
49. Utah 1.03% 1.06% up 4.3% 4.7%
50. South Dakota 0.98% 0.94% down 2.4% 2.7%
Beside from the obvious fact that the five worst states are all run by Democrat Governors and the five best state are all run by Republicans, these are my observations:
The five worst states show a rising death rate, even though the test rate is increasing. The five best state show a falling death rate, which is to be expected as testing is increased.
Michigan has a Detroit problem. The COVID-19 death rate there is over 10%, many got turned away from the few hospitals and were sent home without first being tested. Governor Gretchen Whitmer seems more interested in controlling the healthy population than to protect the vulnerable.
Why Connecticut is second on the list I don’t know, but Hartford County has a problem with a death rate over 10%. It is also next to New York, where the death rate in New York City still is either 7.92% or 10.7% if you include probable deaths.
The problem with New York is that Governor Cuomo ordered nursing home facilities to accept COVID-19 patients, they are not set up to handle highly contagious patients, and so the infection and death rate among the most vulnerable population skyrocketed. One interesting statistics is that two thirds of all New York COVID-19 cases were from people staying home, not going out at all.
The problem with Louisiana is that it let Mardi Gras proceed, people came, did their thing and went back to where they came from, often to under-served areas.
New Jersey is next to New York. Need I say more?
On the other hand, the five best states concentrated their efforts to protect the at risk people, concentrating on hygiene and social distancing rather than trying to micromanage the healthy population. There seems to be no improvement in the outcome by adding testing. In addition the death rate among the five worst states is still rising, whereas the death rate in the five best states is declining.
Governor Kristi Noem of South Dakota, the state with the best outcome of all states so far did order a clinical test of using the combination Hydroxychloroquine + Azithromycin + Zinc for five days and that may be the reason the death rate is less than 1 percent. Unfortunately the FDA is concerned that hydroxychloroquine and chloroquine are being used inappropriately to treat non-hospitalized patients for coronavirus disease (COVID-19) or to prevent that disease. Quote:” We authorized their temporary use only in hospitalized patients with COVID-19 when clinical trials are not available, or participation is not feasible, through an Emergency Use Authorization (EUA). These medicines have a number of side effects, including serious heart rhythm problems that can be life-threatening.”
Here is my suggestion: Issue an executive order opening up a clinical study in the effectiveness of COVID-19 treatment with Hydroxychloroquine + Azithromycin + Zinc for five days, and open it up to any qualified Physician or Nurse Practitioner who want to participate. They do the heart test, check for other ailments and report the results to a central data base and a follow up report, and even if it is not a double blind study, once you have a million or so results the FDA can approve the medication. In the meantime over 90% of the patients were getting better, and hopefully nobody had given it to patients with severe preexisting heart conditions. The risk is minimal. It is already approved for Lupus, Rheumatism and Malaria, and the same protocol should apply here.
It is very important the drugs are administered as early as possible. By the time the patient is admitted to a hospital it may be too late. Especially if the patient is already on a ventilator it may do more harm than good.
Why is this study even necessary? This medication is too cheap, it is generic, so no pharmaceutical company is willing to foot the bill on something unprofitable, so it must be done by a university or through a government agency.
It is not that daring a thing to do. Here is a result of a COVID-19 study with more than 6,200 physicians in 30 countries.
- The three most commonly prescribed treatments among COVID-19 treaters are 56% analgesics, 41% Azithromycin, and 33% Hydroxychloroquine
- Hydroxychloroquine usage among COVID-19 treaters is 72% in Spain, 49% in Italy, 41% in Brazil, 39% in Mexico, 28% in France, 23% in the U.S., 17% in Germany, 16% in Canada, 13% in the UK and 7% in Japan
- Hydroxychloroquine was overall chosen as the most effective therapy among COVID-19 treaters from a list of 15 options (37% of COVID-19 treaters)
- 75% in Spain, 53% Italy, 44% in China, 43% in Brazil, 29% in France, 23% in the U.S. and 13% in the U.K.
- The two most common treatment regimens for Hydroxychloroquine were:
- (38%) 400mg twice daily on day one; 400 mg daily for five days
- (26%) 400mg twice daily on day one; 200mg twice daily for four days
- Outside the U.S., Hydroxychloroquine was equally used for diagnosed patients with mild to severe symptoms whereas in the U.S. it was most commonly used for high risk diagnosed patients
- Globally, 19% of physicians prescribed or have seen Hydroxychloroquine prophylactically used for high risk patients, and 8% for low risk patients.
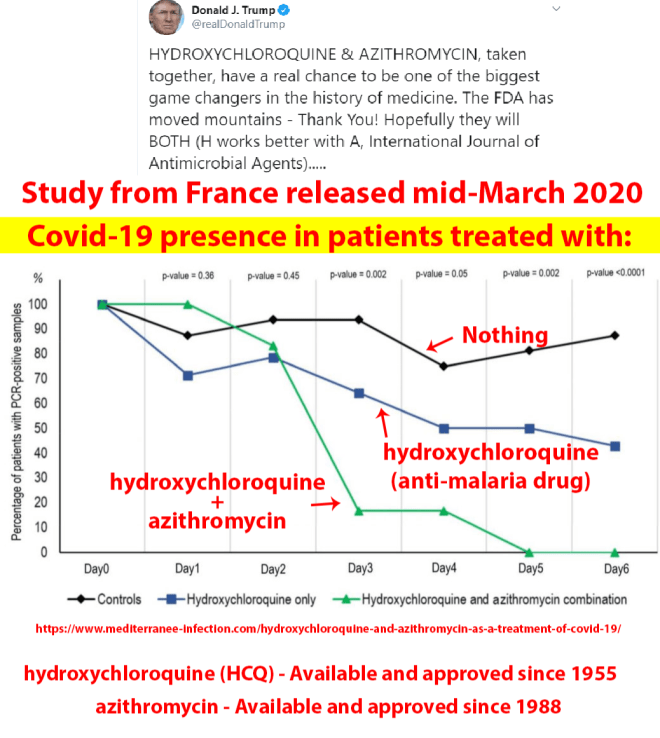
And this is a very recent tweet from president Donald Trump, without which frequent and persistent recommendation this drug combination would have already been approved, as it is in at least 12 other countries.