Washington (CNN)Dr. Anthony Fauci said in May that data shows hydroxychloroquine is not an effective treatment for the coronavirus, disputing use of the drug to fight the deadly virus even as President Donald Trump touts it as a potential cure and says he has taken it himself.
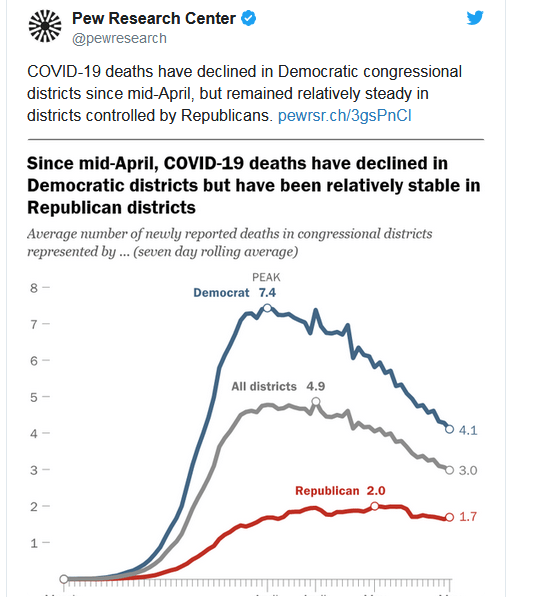
This is a very interesting chart:

But wait. Not so fast. These countries may have a younger population, and the death rate is much lower for younger people. This chart tells the relative death rate, and it shows that with the advent of the coronavirus the death risk doubled regardless of the age of the victim.

The death rate doubles for every 8 years as you age or about 9% per year. The world median age is 30.4 years. So let the world death rate be the norm
World death rate as of June 11 is 5.58% of diagnosed cases. and recovered cases versus deaths is 9.06
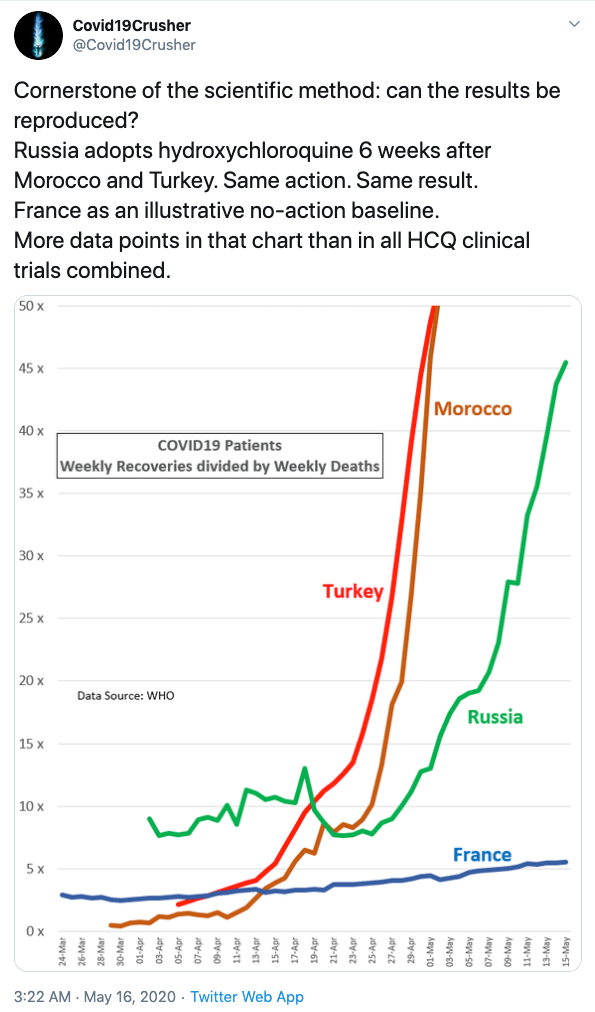
Compare this with 10 countries that use HCQ for most patients as soon as they test positive for the corona virus.
Turkey: Death rate 2.73%, median age 30.9, adjusted death rate 2.62%, recovered cases versus deaths 31.0,
South Korea: Death rate 2.30%, median age 30.9, adjusted death rate 2.21% recovered cases versus deaths 38.5
Malaysia: Death rate 1.41%, median age 28.5, adjusted death rate 1.68% recovered cases versus deaths 59.9
Senegal: Death rate 1.15%, median age 18.8, adjusted death rate 3.08%, recovered cases versus deaths 54.4
Costa Rica: Death rate 0.78%, median age 31.3, adjusted death rate 0.73%, recovered cases versus deaths 60.1
United Arab emirates: Death rate 0.70%, median age 30.9, adjusted death rate 0.68%, recovered cases versus deaths 88.2
Bahrain: Death rate 0.2%, median age 32.3, adjusted death rate 0.2%, recovered cases versus deaths 337.9
Morocco: Death rate 2.47%, median age 29.3, adjusted death rate 2.71%, recovered cases versus deaths 35.9
Russia: Death rate 1.30%, median age 30.9, adjusted death rate 1.24%, recovered cases versus deaths 40.0
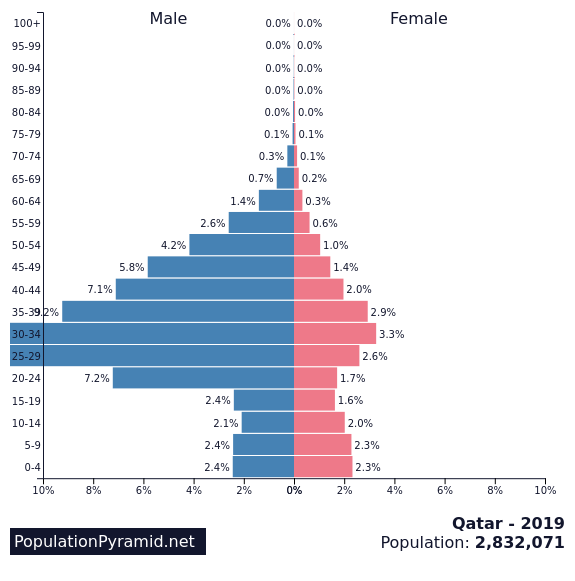
Qatar: Death rate 0.09%, median age 30.9, but since 88% of the population are migrant workers between 20 and 60, the adjusted death rate is at least 8 times higher, or 0.73 %, and recovered cases versus deaths 744.0
Taking the average, not adjusted for the size of the populations we get the average adjusted death rate for countries, where people are taking HCQ + Zinc when diagnosed positive, is 1.59%.
This means that the risk of death is reduced by a factor of 6.0 if HZQ + Zinc is taken as early as possible after a positive diagnosis for coronavirus!
Recovered cases versus deaths is an indicator of how fast patients recover after taking HCQ. Taking the arithmetic average would be unfair, so here I show the median recovery ratio, or about 57, compared to the recovery rate for the rest of the world of 7.05, an improvement of 8.0 times as many recorded recoveries for every death.
What are we waiting for, and what is your concern, Dr Fauci? Hydroxychloroquine is approved for Malaria, Lupus and Rheumatoid Arthritis, and is used by millions or people world wide with normal precautions. It is prescribed for pregnant women and nursing mothers. There are side-effects, but death is not one listed, and the cardiac concern is taken care of with a simple ECG, disqualifying less than 1% of the patients.
WHO paused a double blind study out of an “abundance of caution”.
HCQ was taken by over 800,000 patients testing positive for the coronavirus as soon as symptoms arose or shortly thereafter. We do not need a double blind control study, the results speak for themselves.
Is it because it is promoted by President Trump, and some would rather die than get cured?
Is HCQ too cheap to promote?
I for one want to save lives and suffering.