The headlines say it all. These are the results so far of adverse reactions to various medications and vaccines according to the official VAERS reporting, which give low estimates. The truth is worse. This is from Sen John Johnson:
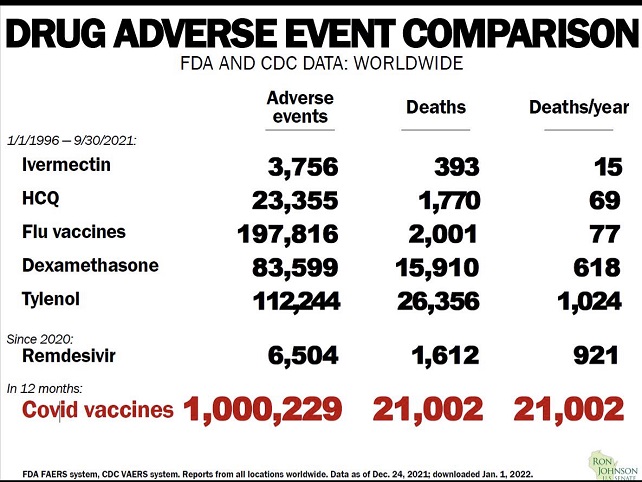
It should be noted that for the first five medications the time frame is nearly 16 years, the result for COVID vaccine is one year.
Of all medications that actually works against COVID with a more than 75% efficiency, Ivermectin has been approved for human use against river blindness and other parasites, such as head lice since late 1980’s. The countries in Africa that routinely use it for parasite control have a COVID case and death rate of less than 1/10th of the countries in Africa that don’t. There are almost no adverse reactions.
HCQ is almost as good COVID fighter as Ivermectin when taken early in conjunction with Zinc. It’s effectiveness is at least 65% and has been used for over 50 years as an anti malaria drug, against lupus and some rheumatoid diseases. It is given to pregnant women and nursing mothers without restrictions.
Flue vaccines have very few adverse effects, but they happen.
Remdisivir was approved very fast, after all, it was expensive and showed early promising results, but it turned out that nearly 30% of the test clientele had used HCQ before entering the protocol. It turned out, that without HCQ it was not so good after all.
Alone in the history of vaccines has COVID vaccines been approved with such a staggering rate of adverse reactions and over 20,000 deaths from the vaccine in a year. Yet it helps people at risk, people over 60, obese, diabetic, anemic, vitamin C and D deficiency, immune compromised, high blood pressure and a variety of diseases, so they were important in the beginning of the disease, and will be for a while until the therapeutics are approved.
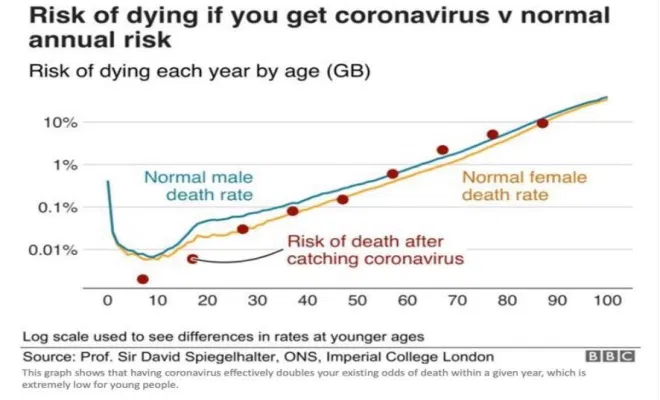
In the mean time , children and young adults without additional risk factors are at higher risk of dying if they take the vaccine than if they get COVID, older people should still go the vaccine route. With admittedly limited statistics available I have calculated the crossover point to be 45 years for people without additional risk factors.